Elderly persons with haemophilia (PWH) commonly suffer haemophilic arthropathy (HA) in four or five joints and have often experienced this from adolescence [1]. Pain in the lower extremities interferes in particular with essential functions such as standing, walking and running, and can be measured on an individual level. In developed countries, elective orthopaedic surgery should be considered in cases where conservative treatment is no longer effective in enabling individuals to perform routine daily activities, and their quality of life and ability to engage in social activities is at stake.
Multiple joint procedures (MJP) were introduced to the clinic at the University Medical Center Utrecht (UMCU) in 1995. MJP are defined as any combination of total knee arthroplasty (TKA), total hip arthroplasty (THA) or ankle arthrodesis (AA) during one hospital admission (one surgical session or staged). Single procedures lead to pain relief in one joint only, implying that limitations in the individual’s ability to undertake activities and participate socially will continue as long as pain in the other arthropathic joints remains. In 2011, we analysed the post-operative clinical rehabilitation [2] of 53 PWH undergoing MJP, revealing 11 subgroups based on different combinations of surgery. A start was made for a core set in order to recommend specific tools for long-term follow-up of this population [3].
The present case series aims to provide insight into individual post-operative changes as a result of MJP, with emphasis on self-reported activities.
Patients and methods
The three cases presented were selected from the group of 53 patients who had undergone MJP at the Van Creveldkliniek, the haemophilia treatment centre at UMCU [3]. Case selection was based on the availability of pre-operative data on activities. Outcome assessment of this study includes two levels of the WHO International Classification of Functioning, Disability and Health (ICF): body (structure and functions) and activity [4]. In addition, assessment of activity level, including self-reported activities, were performed by an experienced physical therapist. An outline of measurement instruments used pre- and/or post-operatively is presented in Table 1.
Table 1
Measurement instruments used pre- and post-operatively per level of the International Classification of Functioning (ICF)
Body functions and structures
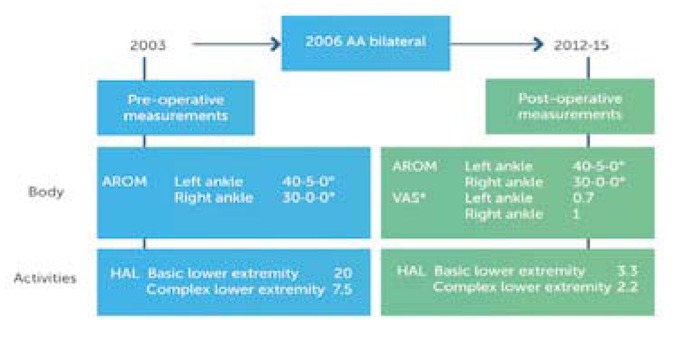
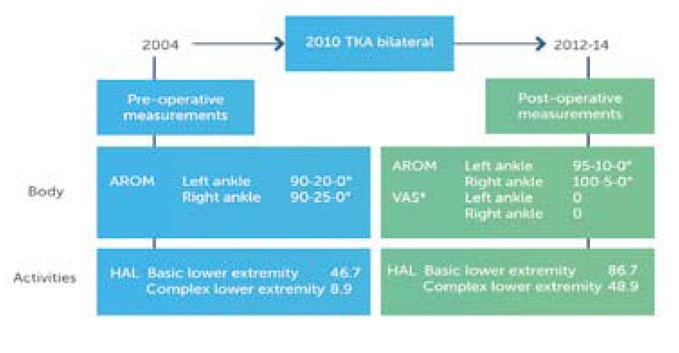
Pre-operatively pain was assessed by the WFH pain score, a four point Likert score (0=no pain, 1=slight pain, 2 = moderate pain and 3 =severe pain) including functional deficit and use of analgetics. Post-operative pain was assessed by a visual analogue scale (VAS) with a continuous scale from 0 (no pain) to 10 (unbearable pain) [3]. Pain was the main indication to perform MJP, but was measured pre-operatively by means of the WFH pain score. To have an approximation of the difference between pre- and postoperative pain, we retrospectively assessed the WFH score, so both pre-and post-operatively.
Active range of motion (AROM) was assessed according to the protocol of the American Academy of Orthopaedic Surgeons [5], as part of the World Federation of Hemophilia (WFH) score [6]. Years of measurements, both pre- and post-operatively, were given in Figure 1 ,2 and 3. All results are given in degrees. And all measurements were in the sagittal plane: for the knee joint flexion and extension, for the ankle dorsal and plantar flexion. The zero transit method was used, whereas the standard neutral position of the knee is zero, and of the ankle 90 degrees.

Activities
Self-reported activities before surgery were measured by a personal inventory, the McMaster Toronto Arthritis patient disability questionnaire (MACTAR – baseline). Part one of this two-part generic instrument, comprising a semi-open interview, was used to identify functional limitations in the individuals’ lives and to prioritise a maximum of five activities causing the most limitations [6]. The MACTAR follow-up evaluated the priority items one by one, asking whether a specific activity cost less, more or the same amount of energy.
The HAL is an haemophilia-specific instrument, validated for use with PWH, in which a score of 0 indicates the absence of and 100 a maximum of functional problems [7]. It comprises 42 questions, divided into seven domains, with each response measured on a six-point Likert scale. As the surgery of the case group focused on the lower extremities only, two domain scores were used: basic and complex activities of the lower extremities before and after surgery. The basic lower extremity subscale contains six item, while the complex lower extremities subscale has nine items [8].
Results
All three cases were males with severe haemophilia A, without an inhibitor, all HCV–RNA positive, who had visited the haemophilia centre at UMCU on a regular basis over several decades. At the time of surgery, the mean age was 57 years (range 48–62). The mean interval from assessment used to surgery was 4.7 years (range 3–6 years) and from surgery to last assessment used was 8.3 years (range 4–9 years). For more than 10 years post-surgery, all three patients have undertaken weekly hydrotherapy for seven months during the winter period.
Post-operative pain assessment scores on the VAS (0–10) was on average 0.3 (range 0–1), indicating minimal pain in all cases. Retrospectively pain improved of all the joints operated on: Case 1: LK 3 and 1 (△= 2) and RK 3 and 1 (△= 3); Case 2: LA 2 and 0 (△=2) RA 2 and 0 (△=2); Case 3: LK 3 and 0 (△=3) and RK 3 and 0 (△=3). The active range of motion of four knees (cases 2 and 3) increased between 5 and 10 degrees, and extension 0 till 20 degrees. As a result of the fixation of the tibiotalar joint, active range of motion decreased in case 1; plantar flexion average 15˚ (range 10– 20˚) and dorsiflexion average 7.5˚ (range 5–10˚).
Self-reported basic lower activities on the HAL showed an improvement (range 20–46.5) in all patients. The scale of this effect over one standard deviation (of 18)[9], i.e. with an effect size of >1, is generally considered to be large [10]. The increase in the score for complex lower activities was less pronounced (range 3.5–40); no data on standard deviations were available for this summary score. The difference of the lower complex activities was evident: cases 2 and 3 increased (figures 2 and 3), whereas case 1 showed an increase. The MACTAR priority lists confirm improved activity levels in each patient - shown in tables 2, 3 and 4 - but individual differences are clearly visible.
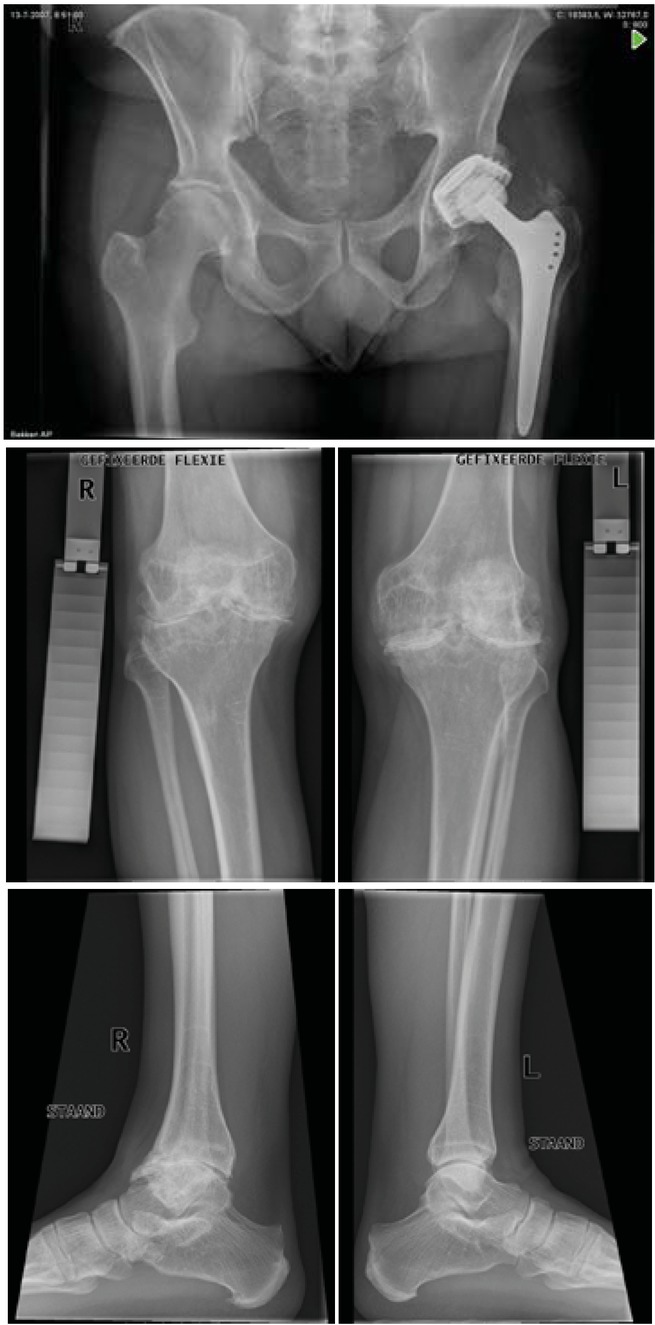
Figure 4
Case 1 X-rays before (2005) and after (2007) bilateral pan arthrodesis by means of an ankle arthrodesis nail in 2006
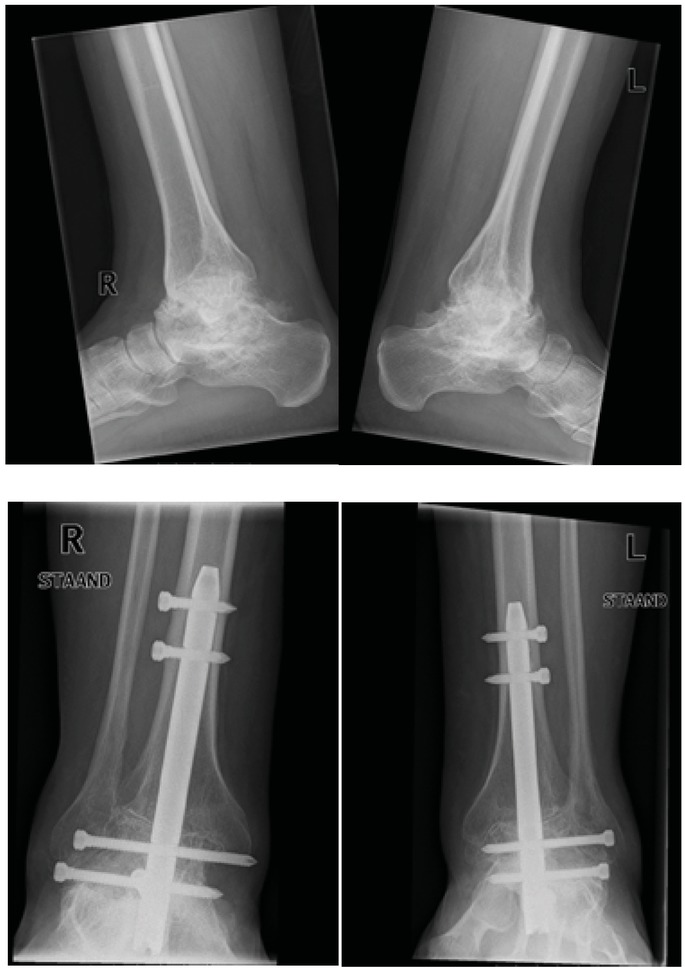
Table 2
Case 1 Top 5 problems (MACTAR)
Table 3
Case 2 Top 3 problems (MACTAR)
Table 4
Case 3 Top 5 problems (MACTAR)
Case 1 – Bilateral ankle arthrodesis
The patient is married with no children and is in regular employment as an ICT expert. He was 48 years of age at time he underwent MJP: in 1990 he has a THA to his left side and in 2000 a THA to his right side. He has several adaptations at home (a stair lift, shower chair, grab bars, removal of all thresholds). Overall, he is able to do more activities, but is sometimes tired (HCV). His knees not being replaced was a hindrance initially, but became less so. He has lately experienced more pain in both knees and further surgery is now planned. The patient’s top 5 problems based on the MACTA questionnaire are summarised in Table 2.
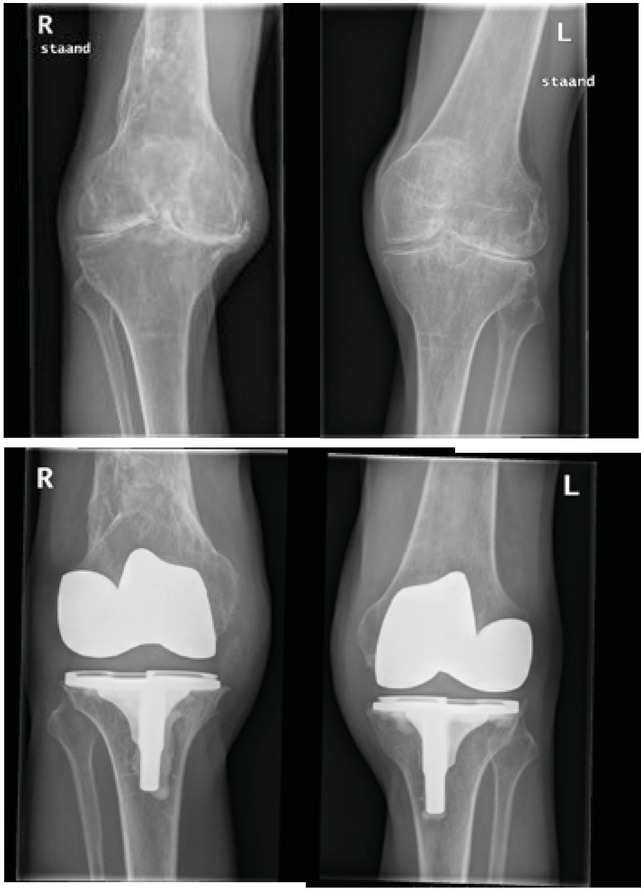
Figure 5
Case 2 X-rays before (2009) and after (2010) bilateral total knee arthroplasty (type Genesis II (centered) with patella button)
While in hospital he developed diverticulitis during the week following AA surgery complicated by perforation. A sigmoid resection was required and a planned bilateral TKA was cancelled. Clinical physiotherapy focused on maintenance of knee joint motion only. He was discharged three weeks after his AA surgery, wheelchair-bound and unable to stand as a result of complications. At home, he receives regular sessions with a local physiotherapist, focused on maintaining AROM in both knees, standing and walking short distances. He also receives hydrotherapy at UMCU. After achieving standing and walking in hydrotherapy. physiotherapy sessions were shifted towards colleagues in the first line care (hometown).
Case 2 – Bilateral TKA
This case is that of a single, unemployed man aged 60 years at time of MJP. He underwent rehabilitation in hospital: physiotherapy focused on AROM for two weeks, standing, transfers and walking (walking aid) until discharge. He was admitted to a rehabilitation centre three weeks post-surgery, where he received daily physiotherapy and hydrotherapy sessions combined in weekly programmes. At home he then received regular sessions with a local physiotherapist as well as hydrotherapy at UMCU. He returned to regular group hydrotherapy sessions after 6 months.
The patient is now very positive and says: -‘’A miracle happened to me’.’ He goes out more frequently and recently played percussion in a standing position for 3 hours. He was riding an adapted bike, with the saddle positioned rearward, as getting on proved easier, but was able to ride a regular bike when his adapted bike was stolen. He has adaptations to his orthopaedic shoes and his ankle pain is slowly progressive.
Case 3 – Bilateral TKA
This patient is a married man with three children and four grandchildren. He is unemployed but active in upholstering on a voluntary basis. In 1995, he has a THA left side.
He recieved rehabilitation In hospital: AROM was regained by active exercise (assisted in the first week) with passive exercise by means of a continuous passive machine (CPM). He was discharged eight days post-surgery. At home, he used two crutches during the first 2 months. He received daily physiotherapy sessions for 1 year, and hydrotherapy (UMC Utrecht) twice-weekly, although this was stopped after a few months. There was very little progression in standing and walking.
Surgery was postponed by the patient himself for too long. Unfortunately, he is unable to ride a bicycle, although he is physically much more active and has more energy: he is very pleased to be able to do activities with his grandchildren.
Discussion
All of these three cases provide insight into the physical consequences of MJP in PWH, with emphasis on self-reported activities, but also on the relationship between the different levels of the ICF. The cases are complementary to two previous articles on this very specific population, describing clinical rehabilitation [2] and the onset of long-term follow-up [3].
Although not representative for the total MJP group – a heterogeneous group consisting of 11 subgroups of combinations of operated joints – the individuals selected for the study represent two of the larger subgroups (TKA bilateral, n=11; AA bilateral, n=9), although inclusion was based solely on the availability of pre-operative functional data. Complications (case 1) are not specific to these particular subgroups and also occurred in other subgroups.
As known from literature, the MACTAR is able to detect changes over time [6], but its main disadvantage is a shift in patient priorities during long-term follow-up [11]. This implies that the period of time between measurements of our cases, often many years, is not ideal. The method of questioning in the official MACTAR follow-up (‘’Does an activity cost less, the same or more energy’’) is probably not the best way to detect differences. In time, especially in a population of elderly PWH, all activities cost more energy (personal statement: case 1). Case 1 also indicated that adaptations in his home influenced the MACTAR follow-up; for example, he now uses a stair-lift when knee pain and swelling are present.
Although MJP is the main intervention, it is important to take account of the role of rehabilitation, and of physiotherapy in particular [2]. As an example, the major complication experienced by case 1 led to a complete physical inability to stand in an upright position. As a start, a standing position could only be achieved during hydrotherapy (upward pressure). Long-term follow-up should not result a total ignorance of short-term results; physiotherapists should evaluate short-term results during rehabilitation, e.g. functional milestones after surgery or acute bleeds. The term ‘functional milestones’ was introduced by Guccione et al. after hip fracture [12]. Latham et al. point to the usefulness of functional recovery through functionally-oriented exercises, even after regular rehabilitation [11]. Unfortunately, the culture of measuring short-term effects in a structured way is not yet widely present in physiotherapy practice (AM Jette, personal communication), nor is there sufficient natural interest in data [13] – but this is exactly what the profession needs. The ICF level of activities, however, is the ultimate level for physiotherapists to measure and prove their professional results, and thus the benefits for the patients, which became clear in these case studies. In this study results only two ICF levels are presented, but the authors are aware that participation, as well as environmental factors are key as well. After all, all these patients made this big effort with as a main goal release of pain and continue participation in their own society and environment.