Acquired haemophilia A is a rare autoimmune bleeding disorder that can result in life-threatening haemorrhage. It is caused by the spontaneous development of autoantibodies that attack factor VIII, neutralising coagulation activity. Neutralisation causes factor VIII levels to decline, leading to haemorrhage, characterised by subcutaneous and muscle haematoma [1]. Where haemostatic management of acquired haemophilia is required, bypassing agents such as FEIBA (Factor Eight Inhibitor Bypassing Activity) should be used as response to factor VIII concentrate is poor [2].
In the United Kingdom there are a reported 1.48 cases of acquired haemophilia per million people per year [3]. The incidence of acquired haemophilia seems to increase with age, and is more common between 65-85 years of age [3]. Specialist investigations are required in order to diagnose it [4].
Kinesio tape was invented in Japan in 1973. It is designed to influence muscle and soft tissues while still allowing full range of movement [5]. Kinesio tape can be used for a variety of different functions depending on the desired outcome: the author has used it with good results in the acute sports setting to treat muscle strains and bleeds.
Kinesio tape is used in all aspects of physiotherapy but there is no published evidence of its use in haemophilia. However, as patients with haemophilia and other bleeding disorders present with swelling during a bleeding episode, there is a rationale for using Kinesio tape lymphatic drainage technique in these patients.
Presenting case
A 73-year-old woman presented with a swollen and bruised left leg that had been worsening over the past few days. Symptoms started spontaneously and there was no reported trauma. Prior to hospital admission she suffered several small bleeds, before presenting with a large bruise on her left thigh that spread into her left calf, a few days before diagnosis. This delay in diagnosis in the presence of symptoms could have put her at risk and increased the potential for bleeding [3]. A few months prior to presentation she had been diagnosed with hyperthyroidism and type 2 diabetes.
Examination of the left leg revealed high levels of pain with movement that measured 7/10 on a Visual Analogue Scale (VAS) and restricted her ability to walk. Range of movement in the left knee was also restricted due to pain and stiffness (flexion 50° and extension -20°). Palpation of the left thigh indicated a large, firm and warm haematoma over the lateral aspect. Straight leg raise was absent. A musculoskeletal bleed was suspected. The VAS and range of movement represent outcome measures for progression.
Investigations
A diagnosis of acquired haemophilia A was made after detecting a prolonged activated partial thromboplastin time (APTT) of 137 seconds, factor VIII level of <0.01 IU/dL, a factor VIII inhibitor titre of 619 BU/ml and a fall in haemoglobin to 79g/L. An ultrasound scan, requested on admission to identify the extent of the thigh bleed, confirmed a left vastus lateralis haematoma, which measured 15cm in length and 1.7cm in diameter.
She had a biochemical hyperthyroidism, negative thyroid peroxidise antibodies, with small multinodular thyroid goitre on CT imaging. Thyroid ultrasound showed a bulky thyroid consistent with thyroiditis and confirmed the presence of several nodules. A diagnosis of thyrotoxic Graves’ disease was made.
Management
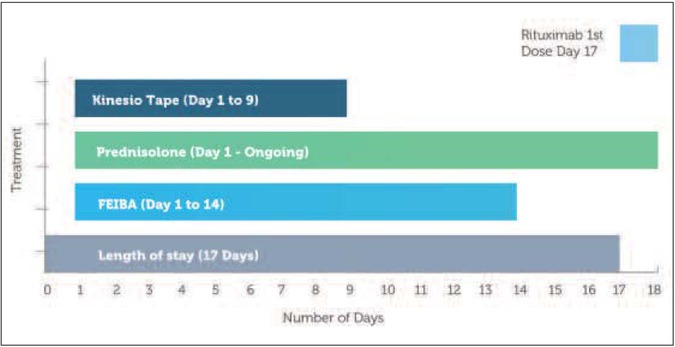
Following the diagnosis of acquired haemophilia A, the patient was started on a course of FEIBA (7000 units twice daily) and prednisolone, in order to control bleeding and eradicate the inhibitor [3]. As the patient had a significant haematoma with a lot of swelling and bruising in the left lower limb, it was decided to use Kinesio tape over the area of bleed in order to try to reduce some of the swelling and improve lymphatic flow, relieve tension and reduce the pain.
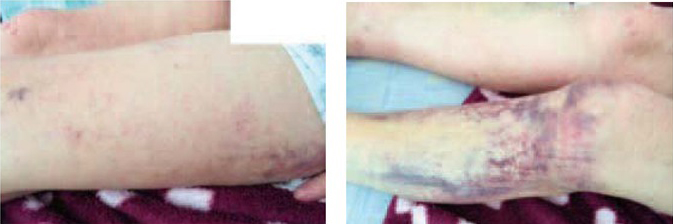
Kinesio tape was applied over the bruising and swelling in the left thigh, which also tracked down into the left calf 24 hours following admission. Figure 1 shows pictures of the left shin and thigh prior to taping. A test tape was performed and the patient did not experience any skin complaints or sensitivities to the tape. No other contraindications to the tape were present and consent to treatment was obtained. Bed rest was also advised.
Figure 1
Day 1, pre-tape and post-tape (right and far right)
• Active range of movement left knee 0-70°, left hip flexion 80° and left ankle full range. Palpation firm and tender over area of bruising left thigh. Warm to touch. Straight leg raise (SLR) and static quadriceps (SQ) weak left side.Sensation intact. Pulses left leg palpable. Visual analogue scale 7/10
• Factor VIII 1.6%; inhibitor titre 619 BU/mL; haemoglobin 79g/L

Swelling causes increased pressure and a lack of skin movement and this increased pressure may inhibit the lymphatic system [6]. The manufacturers of Kinesio tape report that the micro convolutions in the tape gently lift the skin away from the underlying tissue, which in turn releases pressure and allows lymphatic fluid movement [7]. In theory, the stretch on the tape also provides a micro massage that can help redirect fluid to a less congested lymphatic pathway, in this case the groin and behind the knee.
Three ‘fan’ strips were applied to the left thigh and lower leg to clean dry skin, with the anchor of the strips located near lymph nodes in the groin and the back of the knee (Figure 1, right). The tape had a 15% stretch (‘tape off’ tension), which gives a slight recoil effect and is the technique used for lymphatic drainage. The tape covered the area of swelling and bruising in the left leg, crisscrossing the entire area to get maximum effect. The aim of this tape technique was to redirect the swelling to the lymph nodes in a less congested area.
After 48 hours the tape was removed and some of the swelling and bruising around the left leg had reduced (Figure 2). Physiotherapist assessment suggested reduced tension in the soft tissue compared to pre-tape assessment, and a stripy mark over the bruising. It may be that the application of the tape assisted in the drainage of the fluid within the leg by redirecting it away to a less congested lymphatic pathway. Bed rest may also have helped settle the pain, as restricted movement would place less stress on the soft tissues allowing the bleed to settle. However this would not account for all the changes.
Figure 2
Day 3, post-tape and (far right) with tape re-applied
• Active range of movement left knee 0-100° and left hip flexion 80°. Palpation reduced tension left thigh over bruise more pliable skin.SLR and SQ weak left. VAS 2/10
• Factor VIII 2%; haemoglobin 111g/L

The patient also reported reduced pain (VAS 2/10) and an increase in knee range of movement (flexion 100 degrees extension 0 degrees).
At this stage Factor VIII levels were 2%, indicating a clinical response, so FEIBA was reduced to 5000 units twice daily.
As improvements in function and pain had been observed, to maximise treatment the tape was re-applied using the same technique and covering the same target area (Figure 2). The patient was encouraged to start gentle ankle and knee exercises, within limits of pain, to promote circulation.
After a further 72 hours the tape was removed (Figure 3). The patient reported that her pain had settled (VAS 0/10) and range of movement had returned to normal but complained of tightness in the thigh at end of range knee flexion. The haematoma would still have been present in the thigh so stretching the muscle by bending the knee would produce some tightness. Straight leg raise was normal with no restrictions. Physiotherapy assessment identified a further reduction in skin tension with a visible reduction in bruising.
Figure 3
Day 6, post-tape
• Active range of movement left knee 0-140° and hip flex 110° equal to right side. SLR and SQ normal. Palpation left thigh reduced tension spongy feeling. VAS 0/10
• Factor VIII 4%; haemoglobin 112g/L

The patient was advised to mobilise short distances only and the tape was re-applied for the third time due the ongoing improvements in symptoms and function, using the same methods covering the remaining areas of bruising and swelling. A further 72 hours later the tape was removed (Figure 4). At this point all bruising and swelling from the upper thigh had receded and the patient reported no pain or restriction to mobility, although she did complain of tightness at end of range flexion. On palpation of the lateral aspect of the thigh a small haematoma was present, which would account for the stiffness within the muscle.
Figure 4
Day 9, post-tape
• Full active range of movement left lower limb with residual stiffness in the left thigh. SLR and SQ normal. Palpation left thigh slight haematoma so evidence of swelling. Resisted Quadriceps 5/5 Oxford scale. VAS 0/10
• Factor VIII 4%; haemoglobin 112g/L
Physiotherapy assessment showed some residual bruising around the shin, tracking down the leg but no skin tension was present: stripy marks remained visible in the bulk of this bruising. At this stage factor VIII levels were 0.03 IU/dL and FEIBA was further reduced to 3000 units twice daily.
The patient was started on a basic exercise program to help strengthen and stretch the muscles of the lower leg.
The quadriceps had been inhibited by the thigh bleed and as symptoms were improving exercises were started to stretch and strengthen the area, and to help return the muscles to their pre-bleed function. No further tape was applied to the thigh as the patient was discharged home over the weekend with a 10-day follow up, leaving it difficult to monitor the tape. Upon discharge her factor VIII level was 8% and FEIBA was stopped due to the significant clinical changes in bleeding patterns.
Outcome and follow-up
The patient was discharged after 17 days in hospital. Prior to discharge, a first dose of rituximab (an immunosuppressant used to control the production of antibodies, which helps to maintain factor VIII levels) was administered as an inpatient with two further weekly doses administered as an outpatient. Following this treatment factor VIII level rose to 74% and the rituximab was discontinued, with the patient asked to attend clinic every three weeks for monitoring of factor VIII levels.
The thigh bleed has completely resolved and patient is independently mobile and managing well with no more stiffness at end of range knee flexion. Following her last appointment, 56 days after admission and diagnosis, her factor VIII level was 108%.
Discussion
In this instance, the use of Kinesio tape in conjunction with FEIBA and prednisolone appeared to assist with the management of the patient’s bleed, reducing swelling and pain and facilitating the patient’s return to normal function.
Kinesio tape is claimed to facilitate myofascial release and increase the re-absorption of lymphoedema in underlying tissues [5]. The need for further investigation for this treatment technique in patients with haemophilia is clear.
The use of Kinesio tape to promote lymphatic drainage has been researched in mastectomy patients with lymphoedema [8]. Lymphodema following mastectomy and removal of lymph nodes is common due to the adverse effects of treatment on the operated arm. The study followed women over a 20-day period post-mastectomy using elastic therapeutic taping with no comparable treatment. The results indicated the tape considerably reduced swelling and increased shoulder range of movement contributing to an overall increase in local muscle strength. These findings were confirmed by two studies in which Kinesio tape was used as an alternative treatment for breast cancer patients with lymphoedema [9,10]. However, there is a need for more clinical trials investigating the effectiveness of Kinesio tape for lymphatic drainage.
Improving lymphatic fluid flow with the application of tape, by redirecting fluid to a less congested lymphatic pathway around the soft tissue bleed up the hip and behind the knee, could potentially accelerate the recovery process. The inguinal and femoral lymph nodes in the groin and the popliteal lymph nodes behind the knee were used as markers for the tape. The lymph nodes in the hip were above the area of swelling so would be less congested. The tape provides micro massage to the skin, which may help natural drainage via the lymph nodes. The superficial lymph vessels lying between the superficial fascia would transport the swelling to the lymph nodes to be absorbed.
After eight days the thigh had reduced in size and resembled the contralateral side. Unfortunately, no measurements were taken so this is based on visual feedback and palpation of the thigh.
Kinesio tape has been reported to have an impact on pain by improving lymphatic flow and reducing the pressure with the soft tissue [5] and in this case the patient reported improved pain levels soon after initial application of tape. Two days after application, her pain was 2/10 VAS; five days after initial application, the patient reported that symptoms had settled and pain was no longer present (0/10 VAS). The aim of using the tape is to lift the skin reducing pressure around the thigh caused by inflammation within the soft tissue, which would help reduce levels of pain.
Range of movement in the knee increased steadily following the application of Kinesio tape. Five days after initial application, the range of movement in the left knee had returned to baseline, equalling the right knee. Straight leg raise was normal and quadriceps function returned to normal (5/5 Oxford scale). The patient’s function responded quickly despite the size of the initial haematoma. This could be due to initial bed rest, gentleexercises, FEIBA or the Kinesio tape.
The subcutaneous nature of the thigh bleed may explain the improvement made with the Kinesio tape, as the bleed is in close proximity to the tape. Deeper muscle bleeds may react differently and improvements may take more time. No damage to the muscle was indicated on the ultrasound scan.
Kinesio tape aims to enhance muscular, joint and circulatory function, which could reduce the duration of treatment required for the bleed. However in this single patient case study it is difficult to quantify whether return of normal function, reduced swelling and pain free movement was in any way facilitated by the application of Kinesio tape: the recovery of this joint bleed may have followed the same pathway and timescale of recovery without the use of Kinesio tape.
Nevertheless, it is possible that Kinesio tape combined with factor replacement therapy may play a role in the management of musculoskeletal bleeds in haemophilia and other bleeding disorders, resulting in reduced length of treatment due to faster recovery, facilitating earlier discharge and potentially resulting in cost savings. This case study has highlighted a need for further investigation in this field of practice.
