Haemophilia B (HB) is a congenital disorder resulting from lack of factor IX, which results in bleeding. Bleeding into joints can lead to chronic pain and disability, while severe spontaneous bleeds, especially in the brain or abdomen, can be life-threatening [1]. Prophylactic replacement of the missing factor can prevent bleeding events and is the standard of care recommended by the World Federation of Hemophilia (WFH) for those with severe and moderate disorders.
Combined with comprehensive haemophilia care, prophylactic factor replacement enables people with haemophilia (PwH) to live an improved quality of life, with near-normal life expectancy [2]. Nevertheless, surgical procedures or other invasive interventions may still be required, whether for haemophilia-related complications or for long-term conditions, such as cancer and heart disease. Surgery is traumatic and is associated with a risk of peri and post-operative bleeding in PwH, requiring specialist care that includes monitoring of factor activity levels, administration of additional factor, and the support of a multidisciplinary team (MDT). Haemophilia clinical nurse specialists (CNSs) working in comprehensive care centres play an important role in coordinating the surgical process within the MDT and in preparing patients for surgery [3,4].
Guidelines published by WFH provide recommendations for factor levels to be attained during major and minor surgery, and during the preoperative and postoperative periods [1]. However, attaining these factor activity levels with standard half-life (SHL) factor replacement products may require continuous infusion or frequent dosing bolus injections to maintain perioperative haemostasis [5].
In recent years, the introduction of extended half-life (EHL) and recombinant factor IX (rFIX) products has optimised prophylaxis by decreasing dose frequency, increasing treatment compliance, and enhancing quality of life without compromising safety and efficacy [6,7,8]. In clinical studies, these products have also been shown to be beneficial in those undergoing surgery [9,10]. This paper reports on the experience of using EHL FIX products during surgery in a small cohort of people with haemophilia B (PwHB) and considers how this has altered the nature of the care provided by haemophilia nurses.
METHODS
A consecutive series of PwHB who underwent minor and major surgery between January 2018 and December 2022 and who received EHL FIX were retrospectively identified from the Katharine Dormandy Haemophilia and Thrombosis Centre (KDHTC), Royal Free London NHS Foundation Trust database. For each patient, the following variables were retrieved:
patient age at time of first surgery
severity of haemophilia (defined as severe = residual endogenous factor < 1 IU/dL, moderate = 1–5 IU/dL, and mild 5–40 IU/dL)
procedure type
whether day case or inpatient stay
severity of surgery (major surgery defined as any invasive procedure where perioperative treatment with clotting factor expected to be longer than two weeks)
length of hospital stay for inpatient surgery
location of day surgery (local/hospital)
EHL FIX product
total consumption of EHL FIX product.
In addition, comparative data are shown for three patients who received an EHL product and who had previously undergone the same procedure with an SHL-FIX product, recombinant coagulation factor IX (FIX, nonacog alfa, Pfizer).
RESULTS
Between 2018 and 2022, a total of 22 surgeries were performed in 10 patients. Median age at initial surgery was 48 years (range: 16–76 years) (Table 1). Surgery characteristics are summarised in Table 2.
Table 1:
Patient demographics
| PATIENT AGE AT TIME OF SURGERY, YEARS | |
| Mean ± SD | 48.1 ± 16.7 |
| Median (range) | 48.5 (16–76) |
| ETHNICITY, N (%) | |
| White | 10 (100%) |
| Asian | 0 |
| Black | 0 |
| SURGERY TYPE, N (%) | |
| N = 22 | |
| Major | 9 (40.9%) |
| Minor | 13 (59.1%) |
Table 2:
Patient and surgery details
There were nine major and 13 minor surgeries, of which 12 surgeries were orthopaedic. Ten of the 13 minor surgeries did not require a hospital stay.
Total EHL FIX consumption ranged from 5,000 to 46,000 IU for major surgery, and from 3,000 to 13,000 IU for minor surgery. Mean FIX consumption (Table 3) was significantly lower for minor surgeries compared with major surgeries (FIX consumption 6,750 IU vs 15,444 IU; p<.05) and significantly lower for outpatient procedures compared with inpatient procedures (mean FIX consumption 5,666 IU vs. 14,083 IU; p<.05). Mean FIX consumption was numerically (but not statistically) lower for inpatient procedures conducted at the lead site compared with remote sites (10,666 IU vs 15,222 IU for inpatient procedures and 5,000 IU vs 6,200 IU for outpatient procedures; p=ns).
Table 3.
Statistical analysis of variables associated with total FIX consumption
| VARIABLE | MEAN FIX CONSUMPTION IU | MEDIAN FIX CONSUMPTION IU (RANGE, N) | P-VALUE* | |
|---|---|---|---|---|
| Inpatient procedure location | at RFH | 10,666 | 10,000 (9,000–13,000, n=3) | n.s. |
| at other sites | 15,222 | 11,000 (5,000–46,000, n=9) | ||
| Outpatient procedure location | at RFH | 5,000 | 4,500 (3,000–8,000, n=4) | n.s. |
| at other sites | 6,200 | 6,000 (3,000, 8,000; n=5) | ||
| Surgery | Major | 15,444.4 | 10,000 (5,000–46,000; n=9) | p < .05 |
| Minor | 6,750 | 6,000 (3,000–12,000; n=12) | ||
| Procedure | Inpatient | 14,083.3 | 10,500 (5,000–41,000; n=12 | p < .05 |
| Outpatient | 5,666.6 | 6,000 (range 3,000–8,000; n=9 | ||
All surgeries were successfully completed without the need for continuous infusion of FIX, which had previously been the standard of care. For six of the minor surgeries, only one infusion of an EHL product was required, allowing some procedures, such as dental extraction, to be performed at the patient's local dentist rather than within a hospital setting. Seven of the nine major surgeries required an inpatient stay of 1–4 days, requiring 1–3 infusions of an EHL FIX product.
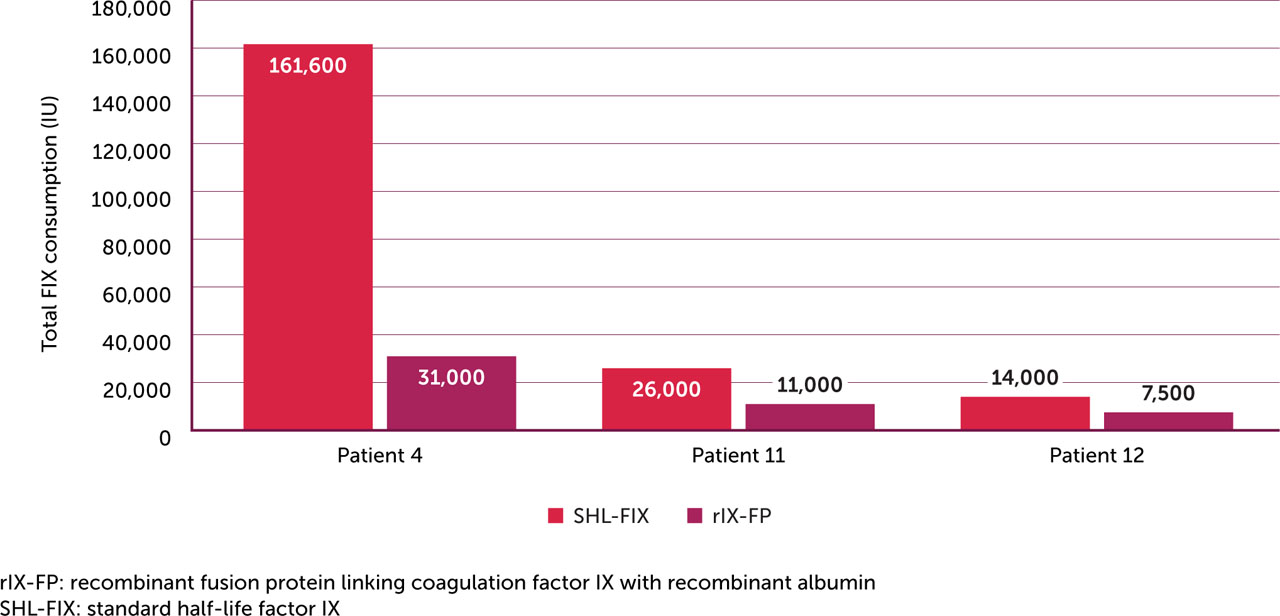
Table 4 and Figure 1 show comparative data for three patients who received an EHL product and who had previously undergone the same surgery with an SHL product. Compared with SHL FIX treatment during the initial surgery, the subsequent surgery under treatment with EHL FIX was associated with shorter hospital stay, no requirement for continuous infusion, fewer factor doses and lower total FIX consumption. The hospital stay during Patient 4's second surgery was prolonged by his home circumstances. The patient's frailty due to his age resulted in a greater need for physiotherapy during his inpatient, and the 15 doses he received included his prophylaxis prior to each every physiotherapy session. Patient 11 had SHL for a prostate biopsy planned as an outpatient procedure but due to increased bleeding post-operatively he required an admission that lasted 3 days.
Table 4.
Product comparison data for three patients who received a SHL FIX product for a prior surgery
DISCUSSION
The KDHTC at the Royal Free Hospital in London is a large comprehensive care centre serving a large population of people with bleeding disorders. This is a very large series of PwHB, which is unusual to see, and it is a good experience for the nursing team in managing surgery in PwHB. In any given week, two or three patients will be scheduled for some form of surgery, principally orthopaedic in nature. While most major surgery takes place on site, some cases are managed in local hospitals, necessitating close liaison with the nursing team in the haemophilia centre. The comparative rarity of haemophilia B means the experience of surgery among PwHB is less comprehensive.
For patients with severe haemophilia B, the product used will be the same EHL FIX product that they use for their regular prophylaxis. For those with mild or moderate haemophilia B, who may be on a standard half-life product, the product is likely to be changed to an extended half-life FIX, in consultation with the consultant in charge of the patient.
As would be expected, inpatient procedures required higher doses of EHL FIX than those procedures carried out as day cases, as did major procedures compared with minor procedures. As a rule, we tend to use higher doses of EHL FIX for those procedures, whether inpatient or outpatient, conducted at remote sites. This is to ensure adequate cover for the procedure itself and to account for any unforeseen delays that may arise remotely.
However, patients are individual and require individualised care that may depend on their home circumstances as well as prior experience. Such factors can make it difficult to make generalisations around FIX consumption. For example, two patients required prolonged stays in hospital for reasons unrelated to haemostasis failure:
Patient No 1 had a dental extraction and remained in hospital for 6 days with complications associated with a dental abscess for which he required intravenous antibiotics. His airway was compromised and was monitored closely in intensive care unit.
Patient No 4, a 76-year-old gentleman who lived alone, had a prolonged inpatient stay of 16 days following a hip revision for which he required rehabilitation and physiotherapy before discharge.
Patient 6 (moderate haemophilia, baseline FIX 3IU/dL) was given EHL FIX for dental procedures involving deep dental scaling. He had previously experienced bleeds following dental scaling undertaken with no cover.
Nevertheless, our findings are in broad agreement with phase 3 study data of EHL FIX products in the surgical setting [9,10]. For example, 30 surgeries (22 major and 8 minor) were reported in 21 surgical patients enrolled in the phase 3 studies within the PROLONG-9FP clinical trial programme for rIX-FP. A single preoperative dose of rIX-FP was used in all but one surgery, administered 3 hours prior to surgery, with haemostatic efficacy rated as excellent or good in 87.5% of minor surgeries and 95.5% of major surgeries. After minor surgery, patients received a median of 0 (range: 0–3) infusions, and after major surgery, the median number of postoperative infusions was 5 (range: 0–11) [12]. In a further study, rIX-FP had a favourable safety profile and was well tolerated when used in major or minor surgeries for perioperative management in patients with severe to moderately severe haemophilia B. Perioperative management with rIX-FP facilitated lower consumption and prolonged dosing intervals compared with conventional FIX replacement therapies, while maintaining the postoperative FIX levels suggested by WFH [13].
From the perspective of the haemophilia CNS, the reduction of injections has decreased the treatment burden for both patients and nurses. The reduced FIX consumption and lower infusion frequency both serve to simplify perioperative care while ensuring optimal protection from postoperative bleeding complications. For patients this means shorter hospital stays or even, in the case of minor surgeries, no admission at all.
The availability of EHLs has made the use of continuous infusion during surgery largely redundant at the KDHTC Royal Free Hospital. This has considerably lowered the workload of the nursing staff, cutting the out-of-hours workload, and easing anxiety around problems with pumps and patients discontinuing treatment. Most patients require only a single infusion of EHL-FIX to cover the procedure and the occasional top-up. Furthermore, peripheral lines are now used much more rarely, reducing the risk of associated complications such as infiltration, extravasation, phlebitis, occlusion, dislodgement and migration, all of which can cause delays to surgery [14]. However, the use of continuous infusion was not common in other centres especially for PwHB, they managed with daily injections even before EHL.
CNSs working in comprehensive care centres continue to play a central role in preparing haemophilia patients for surgery and in coordinating the surgical process [15]. While responsibilities vary depending on the national context, at this centre, the CNS will consider issues around the patient's haemophilia treatment as soon as a patient is scheduled for surgery, e.g., the severity of their haemophilia, whether they self-treat, whether they have any venous access issues, and whether there is a need for a PICC line. As a rule, those patients unable to treat themselves, especially if they have mild or moderate haemophilia, would be given a PICC line and training in how to use it prior to a major surgery.
The CNS will discuss the surgery with the consultant, draft the surgical care plan, and coordinate with the anaesthetist, surgeon and patient and ensure all information is passed on and recorded in the patient's electronic records. They also manage arrangements for measuring pre- and post-surgery assessment of plasma factor levels and ensuring dose adjustment to maintain adequate FIX levels. Where a surgery is scheduled for a local hospital, the nurse specialist will facilitate plans to enable this to happen smoothly, liaising with local nursing staff, the laboratory and pharmacy and whoever is responsible for coordinating medication, organising couriers as needed to ensure the correct factor product is available. Thus, the CNS needs to liaise with:
the named haematologist
the surgeon
the anaesthetist
the theatre and recovery nurse
laboratory staff
the ward nurse
the pharmacy
the data manager
the courier
the patient's family.
Importantly, the CNS places the patient and their family at the centre of all planning, providing education and reassurance as needed. Table 5 summarises the full range of pre- and post-surgery considerations that nurses at KDHTC Royal Free Hospital take into account in order to ensure a safe and satisfactory outcome for PwHB undergoing surgery.
Table 5.
Considerations for clinical nurse specialists when planning surgery
CONCLUSION
EHL FIX products may offer many patient- and centre-related benefits for the care of PwHB undergoing minor and major surgery. EHL FIX allows for intermittent infusions, thus avoiding the requirement for continuous infusions. Furthermore, outpatient treatment may be possible for some minor surgeries in PwHB when treating with EHL FIX products. Reduced dosing frequency and FIX consumption, greater protection from postoperative bleeding complications enabling a better recovery and a shorter hospital stay all reduce demands on medical personnel and could significantly reduce costs associated with surgery in PwHB. Overall, data suggests EHL FIX products can simplify perioperative care in PwHB, with related benefits for the workload of CNSs and treatment centres.