The patient voice is an important consideration in the availability and choice of pharmaceuticals – however, how to capture this complex area and apply it formally within regulation, health technology assessment and reimbursement remains subject to ongoing debate [1,2,3].
The 21st Century Cures Act in the USA highlights the importance of considering the patient experience during the drug development process [4]. The Act facilitates the submission of patient experience information and ‘real world evidence’ to enable more rapid drug and device approval [5]. However, there remains ambiguity surrounding what constitutes real evidence and concerns that overreliance on this data may potentially mislead clinicians and expose patients to unsafe/ineffective treatments [5,6]. Despite these evidential challenges, it is likely that a rise in patient preference data being incorporated in regulatory submissions will be observed moving forward [7].
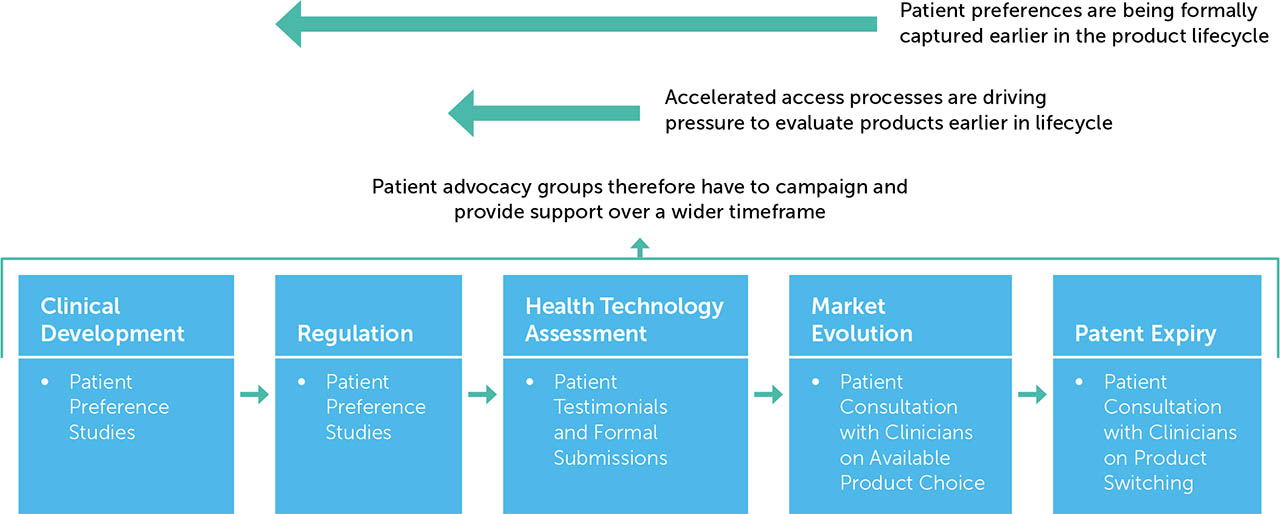
Pharmaceutical regulators such as the Food and Drug Administration (FDA), European Medicines Agency (EMA), and Medicines & Healthcare products Regulatory Agency (MHRA) are accelerating the availability of medicines which target an unmet need [8,9]. Recent examples of this include Project Orbis [10] and the Innovative Licensing and Access Pathway (ILAP) [11]. As health technology assessment (HTA) evolves to meet this scenario [12], accelerated access pathways can also exacerbate the challenge of how to capture patient preferences within HTA and the role patient advocacy groups (PAGs) play within this process. Figure 1 highlights the role played by patients and PAGs in product availability and choice across the lifecycle of a pharmaceutical product. As accelerated initiatives and revised regulatory frameworks will require the formal capture of patient input at an earlier stage, PAGs will have increasing opportunities to campaign and provide support over a wider timeframe.
Figure 1
Impact of regulatory developments on capturing patient preferences across the product lifecycle
Patient preference studies
Patient preference studies can be either qualitative or quantitative and seek to capture the desirability of particular characteristics which are associated with a product in a given healthcare scenario [3]. The Medical Device Innovation Consortium (MDIC) have developed a framework for incorporating information on patient preferences regarding benefit and risk into regulatory assessments of new medical technologies [13]. There is no algorithmic approach to determine which patient preference method to use; method selection is a complex issue which depends on the research question being addressed, the population being studied, and time/budgetary constraints [14]. The MDIC report helpfully provides a catalogue of patient preference methods and groups them by the type of information provided, namely, structured weighting, health-state utility, stated preference and revealed preference [13].
Discrete choice experiments
Discrete choice experiments (DCEs) are a stated preference technique which allows researchers to uncover how individuals value selected attributes of a programme, product or service by asking them to state their choice over different hypothetical alternatives [15]. Stated preference techniques such as DCEs utilise hypothetical examples, typically in the form of a questionnaire, and rely on respondents making choices based on these; revealed preferences analyse patient choices and behaviours in the real world, with examples including patient preference trials or direct questions within clinical trials [13].
A DCE is a quantitative technique for eliciting individual preferences. It is grounded in random utility theory and relies on the assumptions of economic rationality and utility maximisation [15]. This means there is a core underlying assumption that participants can rationally select the choice which gives them the most benefit. The outputs from DCEs show the strength of relative preferences of the characteristics under evaluation and the rate at which they are traded off. The results are often expressed in terms of utilities or marginal rates of substitution. For example, a DCE could investigate the strength of preference for a treatment that is considered more effective than an existing treatment but requires more frequent administration, and the balance between the two that is considered optimal by recipients.
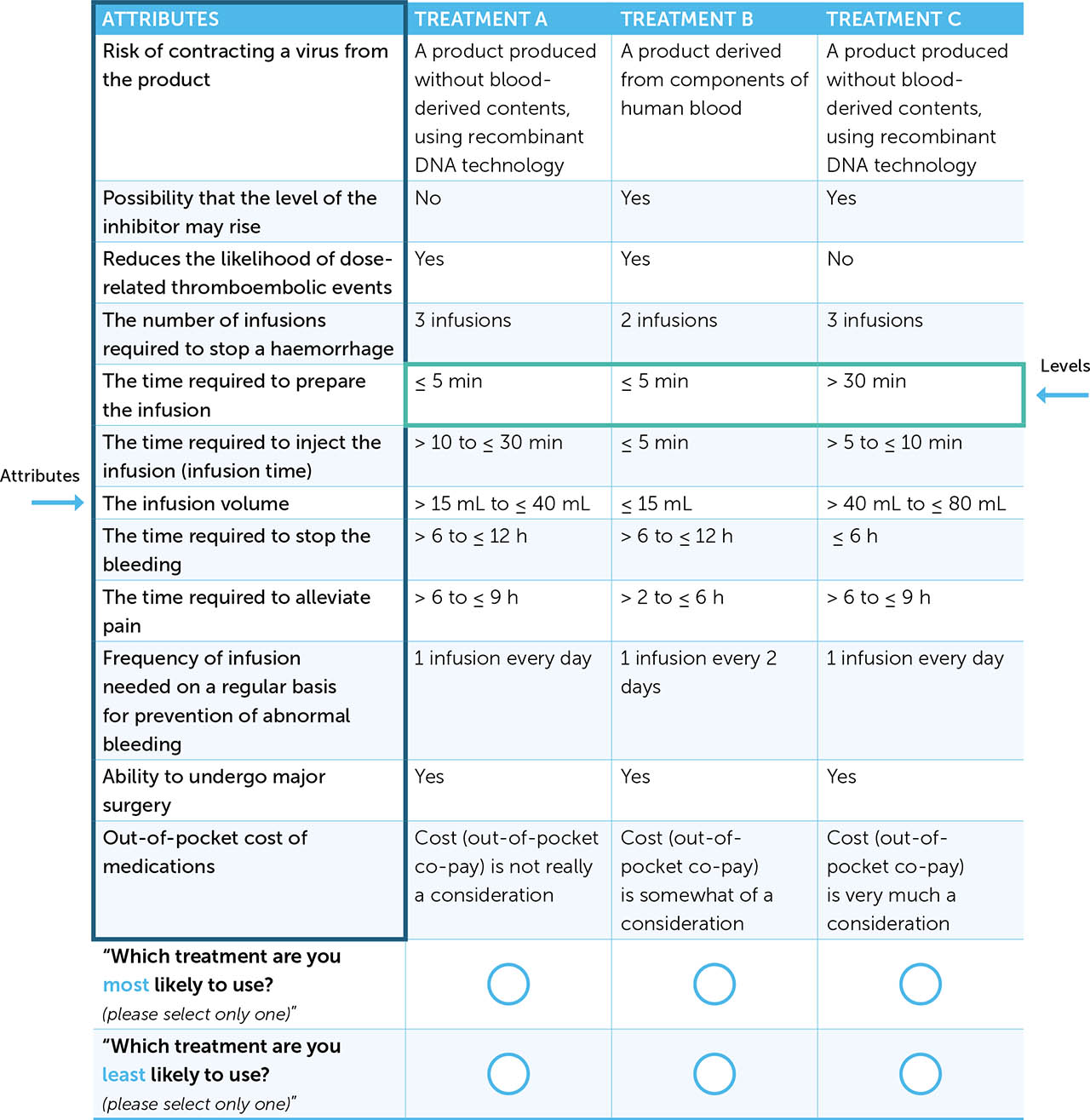
Establishing the attributes and their associated levels is one of the most important and challenging steps in designing a DCE. Attributes represent a technology's key characteristic (e.g. frequency of infusion) whereas levels refer to potential options for a specific attribute (e.g. daily, once a week, once a month). The underlying validity of the study rests on specifying these correctly. Once the attributes are established, the associated levels need to be assigned. These should reflect the range of situations that respondents might be likely to experience [15]. Once the attribute levels are established the next step is to generate a set of hypothetical choice sets [15]. An example from a DCE in haemophilia, with the attributes and levels highlighted, is given in Figure 2 [16].
DCEs are being utilised widely in healthcare and health economics and the method is being used with increasing sophistication in design alongside enhanced analytical techniques which are contributing to a higher quality of output [17,18,19].
DCEs in an evolving haemophilia pathway
Treatment with haemophilia in the mainstream consists of replacement therapy with coagulation factor VIII or factor IX, with a complication being the development of inhibitory antibodies against the infused factor VIII or IX [20]. The journey to the safe and routine infusion of factor VIII and IX therapies has been a challenging one and the freeze-dried powdered concentrates emerging in the 1970s were found to be contaminated by the transmission of HIV and hepatitis C in blood products [21]. As a result of this tragic phenomenon, tighter screening methods were implemented and recombinant (non-plasma derived) technologies were developed [21]. Treatments have continued to evolve in haemophilia with bypassing agents, long-acting coagulator factors, biological therapies and the emergence of gene therapy. Horizon scanning from the Specialist Pharmacy Service (SPS) [22] has recently identified a number of forthcoming technologies in haemophilia (Table 1).
Table 1
Potential future treatments in haemophilia*
| PRODUCT NAME | THERAPEUTIC FOCUS | PRODUCT TYPE | PHASE OF CLINICAL DEVELOPMENT |
|---|---|---|---|
| Serpin PC | Haemophilia A and Haemophilia B | Specific inhibitor of activated protein C (APC) | Phase II |
| Mim8 | Haemophilia A | Next generation FVIII mimetic antibody | Phase III |
| Etranacogene dezaparvovec | Haemophilia B | AAV5 gene therapy (in vivo) | Phase III |
| Fidanacogene elaparvovec | Haemophilia B | AAV8 gene therapy (in vivo) | Phase III |
| Valoctocogene roxaparvovec | Haemophilia A | AAV5 gene therapy (in vivo) | Phase III |
| Concizumab | Haemophilia A and Haemophilia B | Monoclonal antibody directed against tissue factor pathway inhibitor (TFPI) | Phase III |
| Fitusiran | Haemophilia A and Haemophilia B | RNAi therapeutic targeting antithrombin | Phase III |
| Efanesoctocog alfa | Haemophilia A | Fully recombinant factor VIII therapy independent of von Willebrand factor | Phase III |
| Eptacog beta activated | Haemophilia A and Haemophilia B (in patients with inhibitory antibodies to factor VIII or IX) | Transgenically produced recombinant human factor VIIa | Phase III** |
| Giroctocogene fitelparvovec | Haemophilia A | AAV2/6 gene therapy (in vivo) | Phase III |
| Dirloctocogene samoparvovec | Haemophilia A | AAV-LK03 gene therapy (in vivo) | Phase III |
As care pathways such as those in haemophilia become increasingly dynamic, there is a key challenge that patient preferences for advanced therapy medicinal products (ATMPs) in relation to current or future therapeutic options are unknown [12]. Understanding this complex interplay between therapeutic interventions will therefore be vital to inform future healthcare investment decisions. Understanding patient preferences and the impact on uptake of current and future interventions is regarded as a core challenge in budget impact analysis (BIA) and there is an acknowledgement that little data may exist to support assumptions which might be highly sensitive in the assessment [23]. ISPOR guidelines recommend that the mix of interventions over time should be based on past changes, market research, or clinical expert opinion [23]. Whilst sensitivity analysis and a commitment to transparency can assist with the interpretation of BIAs [23], models which rely on historical data, observed uptake of comparable interventions, or expert opinion, fail to account for the dynamic and heterogeneous manner in which individuals make decisions [24]. DCEs could be particularly useful for predicting the uptake of new products where observational data from trials or pilot projects are not available [25], and can potentially improve models that parameterise uptake solely based on expert opinion [24].
METHODS
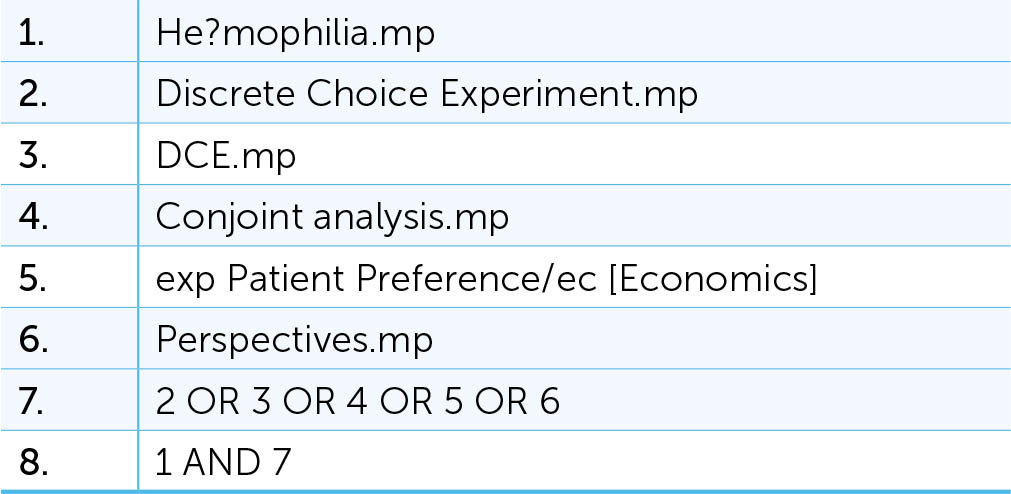
A systematic literature search was undertaken via Ovid MEDLINE and EMBASE CLASSIC + EMBASE with the full search terms set out in Figure 3. Abstracts were uploaded and analysed via Rayyan systematic review software [26].
Articles were included if they concerned a DCE in haemophilia care, if they were a full article, and if they had a pharmacological focus. Articles were excluded for being background information, non-haemophilia specific, biological/other or non-English language.
DCEs in relevant articles were analysed in respect of the audience surveyed, sample size, geography, mean age of patients, format (e.g. paper or online), approach (including extent to which qualitative work supported the DCE, piloting and how these elements were reported), and the attributes and levels per attribute included in the DCE. The study topic and funding source were also documented. Product attributes were mapped over time to investigate temporal patterns.
RESULTS
As set out in the PRISMA diagram in Figure 4, 478 records were identified with 320 records available once duplicates had been removed. A further 200 articles were excluded for being background information (n=146), non-haemophilia specific (n=26), biological/other (n=21) or non-English language (n=7). Of the 120 full-text articles assessed for eligibility, 108 were deemed ineligible due to not being a DCE (n=89), not being a full-journal article (n=18) or not having a pharmacological focus (n=1). This led to 12 full text articles being included, with a date range from 2005–2021 [16,27,28,29,30,31,32,33,34,35,36,37]. The results are summarised in Table 2. This table has been cross-referenced to update previous work conducted on this topic [38]. The review also identified 3 literature reviews [39,40,41] assessing patient preferences in haemophilia, all of which were not full journal articles. There have been two published studies exploring haemophilia patient preferences in relation to gene therapy: one DCE [37] and one utilising a threshold technique [42].
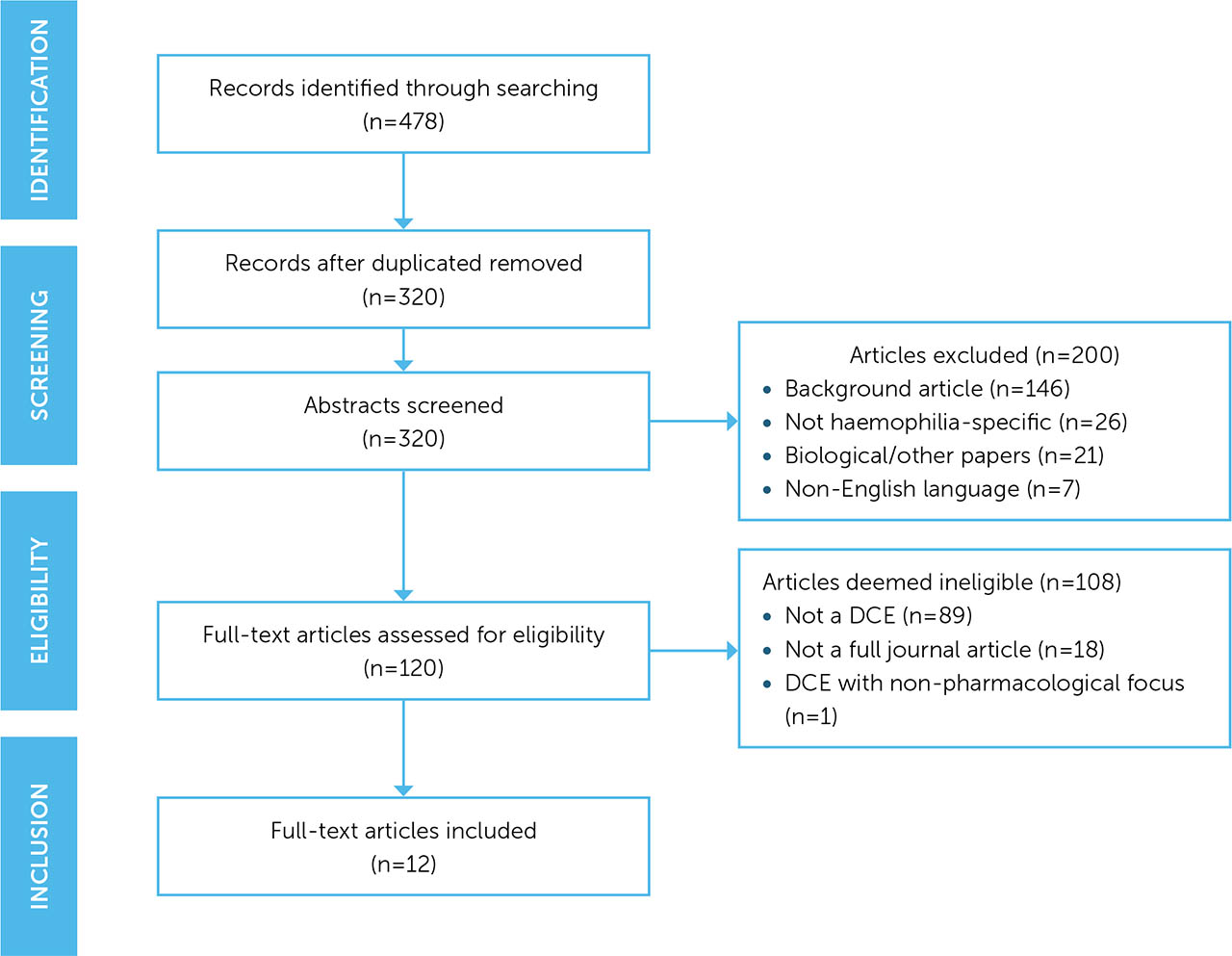
Table 2
Overview of DCEs within haemophilia
| AUTHOR | YEAR | SURVEY AUDIENCE | REGION | STUDY TOPIC | SAMPLE SIZE (N) | MEAN PATIENT AGE (YEARS) | SCALE OF QUALITATIVE WORK | NO. OF ATTRIBUTES | LEVELS PER ATTRIBUTE | INDUSTRY FUNDING | SURVEY METHODS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mantovani et al.[27] | 2005 | Physicians, patients and pharmacists | Italy | Treatment products in haemophilia |
Total: 305 Physicians: 69 Patients: 178 Pharmacists: 58 |
35.9 | Focus group (n=N/R) + Pilot (n=15) | 6 | 2–3 | Bayer Italia S.p.A. | Paper-based survey |
| Lee et al. [28] | 2008 | Physicians | US | Coagulation factor concentrates† | Total: 30 | N/A | Physician engagement (n & format N/R) + testing (N/R) | 12 | 2–4 | Novo Nordisk Inc | Paper-based survey |
| Scalone et al.[29] | 2009 | Physicians, patients and pharmacists | Italy | Coagulation factor concentrates† |
Total: 101 Physicians: 39 Patients: 37 Pharmacists: 25 |
Adults = 41.4 Paedatric = 8.2 |
Focus group (n=N/R) + Pilot (n=35) | 8 | 2–3 | Novo Nordisk Denmark | N/R |
| Brown et al.[16] | 2011 | Patients and caregivers | US | Treatment products in haemophilia† |
Total: 53* Patients: 23 Caregivers: 30 |
20.7 | Used same as Lee et al. (2008)[28] | 12 | 2–4 | Novo Nordisk Inc | Paper-based survey |
| Mohamed et al.[30] | 2011 | Patients and caregivers | US | Treatment products in haemophilia A |
Total: 147 Patients: 77 Caregivers: 70 |
Adults = 38.7 Juvenile = 12.4 |
Face-to-face interviews with adult patients and caregivers (n=8) | 6 | 2–3 | Baxter Biosciences | Web-based survey |
| Gelhorn et al.[31] | 2013 | Physicians | US and EU | Treatment products in haemophilia A† |
Total: 36 Physicians EU: 17 Physicians US: 19 |
N/A | Qualitative interviews (n=4) + Pilot (n=5) | 5 | 3 | Baxter Biosciences | Web-based survey |
| Chaugule et al.[32] | 2015 | Patients and caregivers | US | Willingness to pay for treatment products in haemophilia | Total: 79 | 40.0 | Assistance from Haem author + Pilot (n=5) | 5 | 2–5 | None | iPad at conference |
| Lock et al. [33] | 2016 | Patients, caregivers and HCPs | Multi-country | PK-guided dosing of prophylaxis |
Total: 224 HCPs: 91 Patients: 114 Caregivers: 19 |
38.0 | Qualitative interviews + Pilot (n=10) | 5 | 2–3 | Pfizer | Paper-based survey |
| Fifer et al. [34] | 2019 | Patients and caregivers | Multi-country | Treatment products in haemophilia A |
Total: 54^ Patients: 24 Caregivers: 30 |
N/R | Qualitative interviews (n=10) | 11 | 2–4 | Roche | Web-based survey |
| Su et al. [35] | 2020 | Patients and caregivers | US | Treatment products in haemophilia A |
Total: 209 Patients: 113 Caregivers: 96 |
35.5 | Qualitative interviews (n=10)** + Pilot (n=6) | 6 | 2–4 | Sanofi Genzyme | Web-based survey |
| Park et al. [36] | 2021 | Patients and caregivers | South Korea | Treatment products in haemophilia A | Total: 505*** | 31.5 | N/R | 5 | 3 | Pfizer Pharmaceuticals Korea Ltd | Hospital-based survey |
| Witkop et al. [37] | 2021 | Patients | US | Haemophilia gene therapy | Total: 183 | 38.5 | Qualitative interviews (n=7) ** + Pilot (n=14) | 6 | 3–4 | uniQure Inc. | Web-based survey |
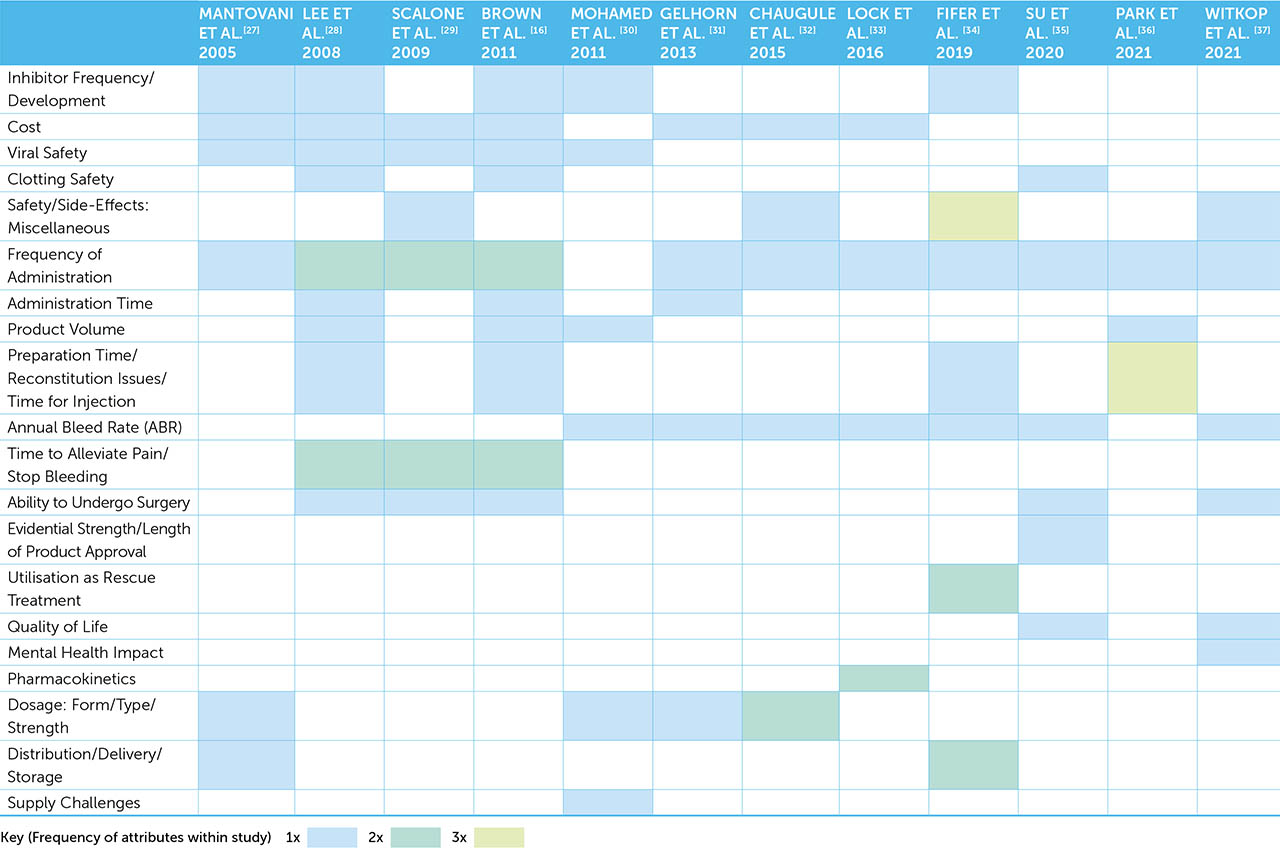
Surveyed audiences included physicians, patients, pharmacists, healthcare professionals and caregivers (either alone or in combination). Two studies focused exclusively on physicians, whilst 50% of the included studies (n=6) surveyed patients and their caregivers. Half of the studies (n=6) were conducted in the US, whilst 3 studies recruited participants across multiple countries. Eleven (92%) studies reported funding by manufacturers with a commercial interest in haemophilia. The sample size between studies varied considerably, with the total sample size ranging from 30 participants to 505 participants. For studies involving patients and their caregivers, the mean patient age range was 8.2–41.4 years; removing the juvenile/paediatric patient population figures narrows this range to 20.7–40.0 years. There was diversity in (a) the scale of the qualitative work undertaken to support the DCEs, (b) the undertaking of pilots, and (c) how extensively this was reported in the included studies. One study did not report undertaking qualitative work [36] and in a number of studies the extent of qualitative work or piloting was difficult to establish. It has been previously reported that inadequate information about methodological detail is hindering assessment of quality [18]. Given the crucial role that qualitative work and piloting plays in establishing the validity of the DCE [15,17], it is vital that future DCEs report the full details of qualitative preparatory work and piloting. Three main methods were employed: web-based, paper-based and in-person survey methods. Whilst paper-based surveys made up the earliest DCEs in this area, there is a clear trend to switching to an online web-based approach, with 3 out of 4 DCEs since 2019 utilising this format. The number of attributes observed per DCE ranged from 5–12, with a median of 6 attributes from the included studies. The levels per attribute was relatively consistent (range 2–5) with 2–3 (n=4) and 2–4 levels (n=4) being utilised most frequently. The development of recombinant products over plasma products was seen as a major therapeutic advance in haemophilia; as shown in Figure 5, a shift of attribute focus from safety towards reduction of bleeding risk has been observed in more recent DCE studies [38].
Head-to-head comparison of gene therapy studies
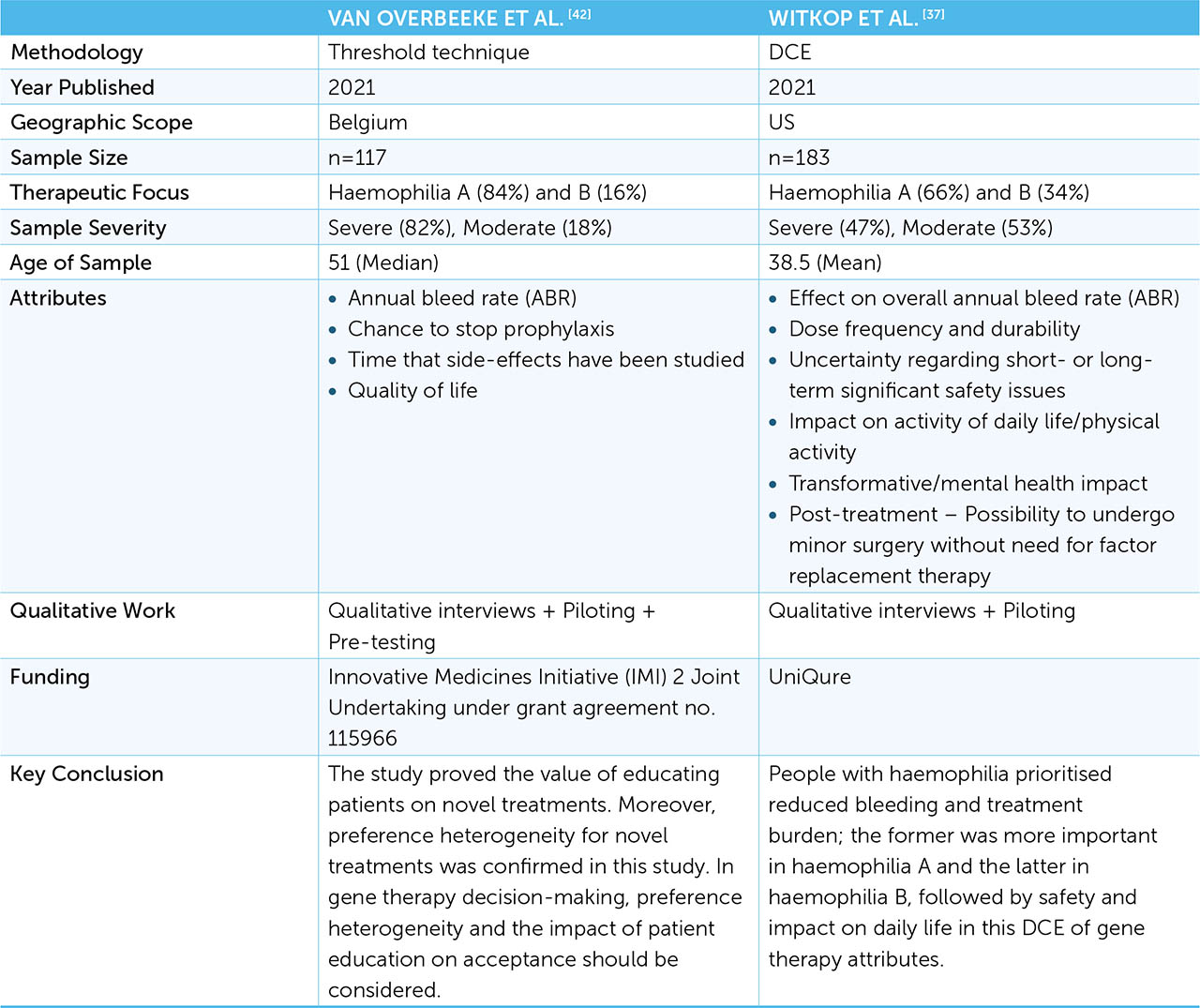
As shown in Table 1, a number of gene therapies are being developed for both haemophilia A and B. Two published studies to date have explored haemophilia patient preferences in relation to gene therapy: one DCE [37] and one utilising a threshold technique [42]. Whilst DCEs have been explored extensively in this paper, the threshold technique is a method that determines the maximal change in one attribute respondents are willing to accept to achieve a given change in another attribute [43]. Van Overbeeke and colleagues ruled out the utilisation of DCE methodology in the development of the study protocol as they estimated that it would be challenging to recruit over 100 participants, which are generally required for DCEs [44]. It is widely acknowledged that method selection is a complex issue [14] and that both methods are stated preference studies that can be utilised to quantify patient preferences [13]. Figure 6 sets out a comparison of the two studies: sample sizes for both were within the range observed with other DCEs to date and, particularly impressive, both studies had to deal with disruption associated with Covid-19. Both studies reported literature reviews, qualitative interviews and piloting to develop and test study attributes and levels. Patients with both haemophilia A and B were included across the studies; sampling in the threshold technique study was aligned to the Belgian haemophilia patient population, whilst over a third of the sampled population in the DCE were haemophilia B patients. Sample severity differed considerably between the studies. The DCE study provided a relatively even split between moderate and severe patients, whilst the threshold technique study had sampling which heavily favoured severe patients. Attributes were consistent between studies with annual bleed rate (ABR), dose frequency, safety issues and quality of life (QoL) being examined, following general trends observed in this area [38]. The DCE also explored the impact on mental health and post-treatment effects. It has been shown previously that training materials result in more choice consistency and facilitate more complex designs [45] and the threshold technique study included an educational tool to assist with understanding of gene therapy. The educational tool was shown to have a significant impact on both the ABR and QoL threshold. The threshold technique study excluded non-factor therapies such as emicizumab, despite 15% (n=17) of the sample being treated with the product.
DISCUSSION
The haemophilia care pathway is constantly evolving, and this phenomenon must be considered carefully when undertaking a DCE to establish patient preferences for product attributes and levels. One of the included studies in the review encountered this issue directly: they were only able to include patients with FVIII administered intravenously, as the subcutaneous emicizumab had not been launched in Korea at the time of patient enrolment [36]. Whilst horizon scanning information is dynamic, and may not be available to all researchers, qualitative engagement with clinicians to future proof study design against pathway changes should be considered as part of the experimental design.
The sample sizes in the included studies varied considerably and recruitment challenges should be actively considered when choosing the study design to capture stakeholder preferences. Methods such as the threshold technique may be more appropriate than a DCE if recruitment to the study will be challenging or the target population is small [44]. One study in the review had a recruitment period of 21 months [34]; as acknowledged in the paper, this length of recruitment may also lead to potential bias.
A recent review highlighted the vital requirement to undertake qualitative research to determine attributes and levels within DCEs, but echoed concerns that inadequate information about methodological detail was hindering assessment of quality [18]. Training materials remain a key but under-developed component of DCEs and the development of interactive tools can potentially improve the quality of choice data if participants are better engaged [45].
There is an increasing trend for DCEs to present attribute descriptions and content using online survey-based methods [45] and videos [46]. One study compared respondents’ understanding of attribute information based on text or video and found that although there was no systematic difference between video or text arms in the study, the information provided by video may better engage survey participants and improve their retention of content [46]. Another study looked at animation training materials, and whilst providing these did not change the preferences of respondents, they did result in more choice consistency which may facilitate more complex experiment designs [45].
A key challenge with DCEs is that they are cross-sectional surveys, which provide a snapshot at a single point of time. This approach has advantages including being inexpensive, simple to conduct and able to reach large audiences rapidly [47]. However, a key limitation is that they are unable to investigate temporal effects [47]. There are a range of temporal and external influences on patient choice including treatment history, family and friends, evolving life situation and clinical opinion, and these factors can change over time, yet the understanding of behavioural impacts on DCEs is currently limited [25,48–49]. Consistency of attributes is likely to be a key issue when considering standardisation of outputs and the routine acceptance of DCE-derived patient data by HTA bodies. Key external events may also heavily influence preferences, for example, after the forthcoming UK report on the infected blood inquiry [50] or a major side effect with an emerging technology, as seen with Covid-19 vaccinations [51].
A key statistic from the review is that all but one of the studies was either directly or indirectly funded by pharmaceutical manufacturers with a commercial interest in haemophilia. If patient preference studies are going to become a formal part of regulatory and pricing and reimbursement submissions, then it is likely that manufacturers will be expected to fund these as part of an evidential package to place before the relevant authorities. Consideration needs to be given on how to standardise the study design/outputs and evaluate quality. The alternative would have to be that PAGs, or independent institutions would have to fill this gap, which may be financially challenging and/or practically unfeasible. Consideration should be given towards a collaborative approach to undertaking DCEs involving multiple pharmaceutical manufacturers to (a) optimise PAG resource and (b) avoid potential suggestions that attributes, and levels, are selected to support individual product benefits.
CONCLUSION
Patient preferences and the methods for capturing these are likely to be subject to ongoing debate as the haemophilia care pathway evolves to offer more therapeutic options with a range of risks and benefits. In addition to challenges with sampling, bias, methodological choice/rigour and manufacturer influence, the question of how best to use the information from patient preference studies remains unclear. Whilst techniques such as DCEs are effective at quantifying patient preferences, they tell us very little about the reasons driving these decisions and the likelihood that they will change in response to temporal or external factors. Given the evolution of the care pathway in haemophilia and the emergence of gene therapy, DCEs could be particularly useful for estimating the uptake of new products and assessing potential budget impact [25]. Several DCE studies in the literature review reported here highlighted the challenge of recruiting participants in rare diseases such as haemophilia, and engaging with PAGs to assist with recruitment is therefore likely to be crucial. Accelerated and reformed regulatory processes are likely to increase demand for patient preference studies and therefore there is an increased requirement to ensure that PAGs are resourced and have the expertise to support these studies alongside other research commitments, and that manufacturers consider collaborative approaches when formally capturing patient preferences.