Haemophilia patients and their families after a training session in Segou, Mali.
A programme of training sessions targeting all relevant stakeholders – including health care professionals, traditional healers, families and media workers – has helped to improve the diagnosis of bleeding disorders in Mali, and provides a model that may be beneficial in other developing countries.

Haemophilia is a rare bleeding disorder that is poorly diagnosed in developing countries. The overall prevalence at birth is estimated at 30 cases per 100 000 male live births [1]. Around the world, approximately 70% of people with haemophilia (PWH) remain undiagnosed and therefore untreated. Among this population, nearly 90% live in developing countries, particularly in Africa [2]. Access to regular treatment with clotting factor concentrates has been shown to contribute to reduced morbidity and mortality in PWH [3,4,5,6,7]. However, despite the efforts of organisations such as the World Federation of Hemophilia (WFH) to improve haemophilia care globally, many African countries face difficulties in initiating haemophilia care programmes. This leads to a high rate of undiagnosed and untreated patients in these countries [8], which in turn results in an increased rate of joint disability and poor quality of life among their haemophilia population [9,10,11].
Efforts to improve haemophilia diagnosis and care in Mali, in sub-Saharan Africa, were boosted in 2012 with the establishment of a national haemophilia patients organisation, the Malian Haemophilia Society (Association Malienne de Lutte contre l’Hémophilie / AMALHEC), which is recognised as a national member organisation (NMO) of the WFH; 20 patients were registered. Following recognition of the NMO by Malian authorities, in 2014 it became part of a WFH twinning programme. Pairing with the haemophilia treatment centre in Montpellier, France, enabled development of local laboratory diagnostics and improved access to clotting factor concentrates.
Improving outreach and diagnosis of people with bleeding disorders is a strategic priority of the WFH. In the Malian context – and in other countries where bleeding disorders are under-diagnosed – we believe that involving the different groups that interact with patients can play a significant role in improving the number of patients diagnosed. This principle was behind the initiation of a project to develop a strategic, collaborative approach to improving awareness and diagnosis of haemophilia in Mali. The project involved the Malian NMO, the WFH, the Novo Nordisk Haemophilia Foundation (NNHF), and other relevant local partners.
Here, we report our experience, and share the challenges faced and lessons learned during the course of the project.
METHODOLOGY
In January 2016, we initiated an innovative two-year prospective study designed to raise awareness and improve the diagnosis of haemophilia and other bleeding disorders in Mali. The study focused on four regions of Mali (Kayes, Sikasso, Segou and Mopti) and the district of Bamako, the capital city. Here, we report the main overall results and detailed results from the Sikasso group.
With the help of the Malian NMO, we sought to promote an integrated approach to building capacity in the diagnosis of haemophilia based on training and awareness-raising, taking into account strategies previously reported in the literature – for example, in a single treatment centre in Senegal and building a national haemophilia treatment network in Brazil – and the standards proposed for economically developing countries [12,13,14,15]. It was also important to consider the local environment and healthcare landscape, and to include all relevant stakeholders.
Those targeted included medical doctors, nurses and laboratory technicians; traditional healers, who continue to play a significant role in healthcare in Mali; opinion leaders and the media; and haemophilia patients and their families. The healthcare department of the Malian armed forces (Services de Santé des Armées) was also included, as it is involved in the treatment and provision of care for both civilian and military patients.
The training sessions were delivered by health care professionals using both oral and video content, and included information about haemophilia symptoms, diagnosis, treatment and complications. The sessions were multidisciplinary. Theoretical training was followed up with practical sessions in the trainees’ hospital laboratory. Learning was enriched by patient testimonials provided by the Malian Haemophilia Society. Before and after each session, the effectiveness of training was determined by formal assessment (10 questions about haemophilia and its management). The sessions were complemented by awareness-raising activities, including public or professional meetings, television and radio broadcasts, and meetings with health authorities, students and media organisations.

Through the training sessions, participants developed a local strategy for identifying people with haemophilia and including them in the national bleeding disorder registry. A suspected case was defined as a patient with a familial or personal bleeding history. Individuals in whom haemophilia was suspected were referred to the district hospital for measurement of prothrombin time (PT) and activated partial thrombin time (aPTT). Alternatively, patients could be identified when routine blood testing revealed coagulation abnormalities – for example, during preparation for surgery. Patients with evidence of abnormal coagulation were then referred to the haemophilia treatment centre to confirm the diagnosis, obtain treatment and join the register of bleeding disorders. With the involvement of the Malian Department for Traditional Medicine (within the National Institute for Research on Public Health, part of the Ministry of Health), we organised special training sessions for traditional healers in each region. They were informed of the study and invited to refer their patients for hospital investigation if signs and symptoms led them to suspect a bleeding disorder.
Involving partners
The training sessions were supported by the Novo Nordisk Haemophilia Foundation (NNHF), the haemophilia treatment centre in Montpellier, France, and the Department of Medicine at the Hôpital du Mali in Bamako. All training courses were facilitated by Malian Health Directorate and the Malian Haemophilia Society.
Anti-haemophiliac clotting factor concentrates were generously provided by the WFH through a humanitarian aid programme.
RESULTS
Training activities
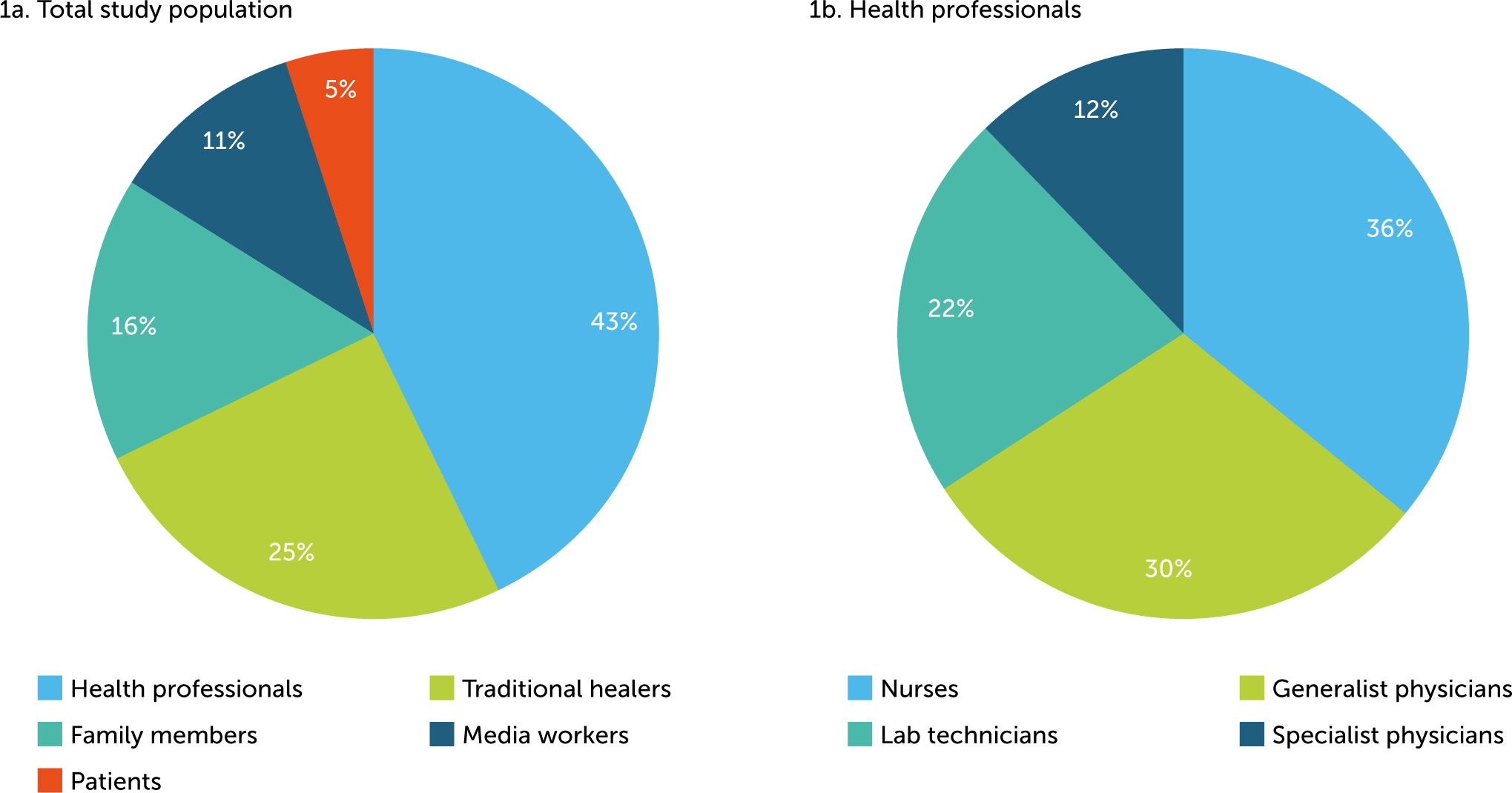
Overall, the programme included 495 participants: 213 health care professionals, 24 patients, 79 parents of patients, 126 traditional healers and 53 media workers (see Figure 1).
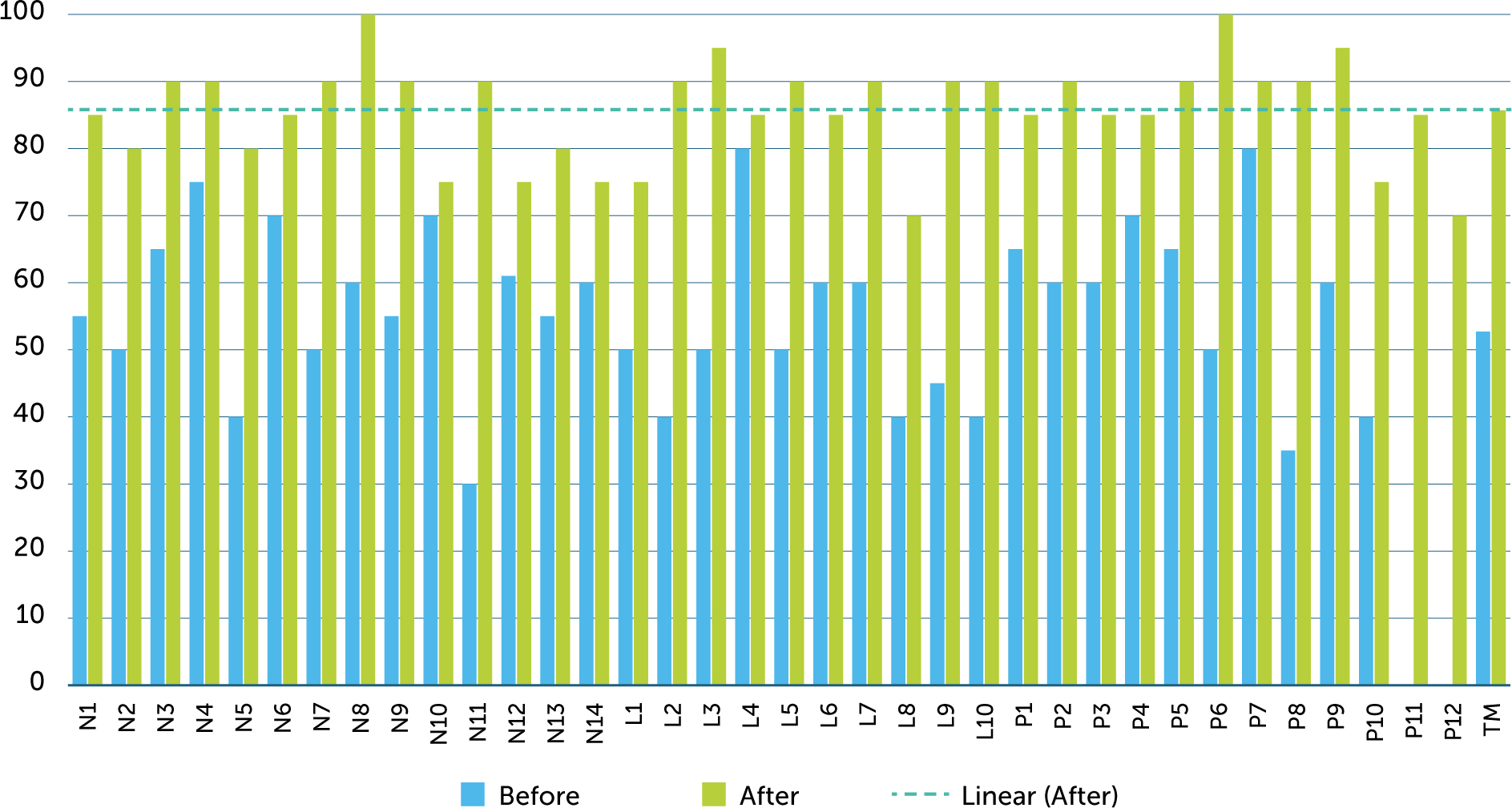
Between January 2016 and December 2017, the programme organised 15 training sessions for health care professionals, five sessions for traditional practitioners, seven sessions for patients and their families, and one session for media workers. Before and after assessments of knowledge in health professionals demonstrated an increase in awareness and understanding of haemophilia. For example, in the session conducted in Kayes, the mean score in the formal assessment was 56.8% before the session and 76.8% afterwards. For the session in Sikasso, the mean scores before and after training were 56.9% and 84.6% respectively for nurses, 51.5% and 86% for lab technicians, and 58.5% and 86.7% for physicians. The scores for health professionals show a relative improvement of around 50–75% (Figure 2).
Impact on clinical activities
The outcome of the referrals is summarised in Table 1.
Table 1
Outcome of referrals
| OF ALL REGISTERED PATIENTS WITH HAEMOPHILIA (N=110) | HAEMOPHILIA A | HAEMOPHILIA B |
|---|---|---|
| Severe | 83 | 1 |
| Moderate | 9 | 5 |
| Mild | 10 | 2 |
Of the 121 patients referred, one did not undergo laboratory testing due to lack of facilities. Eighty-four patients were newly diagnosed with haemophilia. Twenty-nine tests did not confirm a bleeding disorder, and tests could not be carried out in seven patients due to limited laboratory facilities. Traditional practitioners identified seven patients from four families with a suspected bleeding disorder. A diagnosis of severe haemophilia was established in three; tests were unavailable for three and the seventh was lost to follow up.
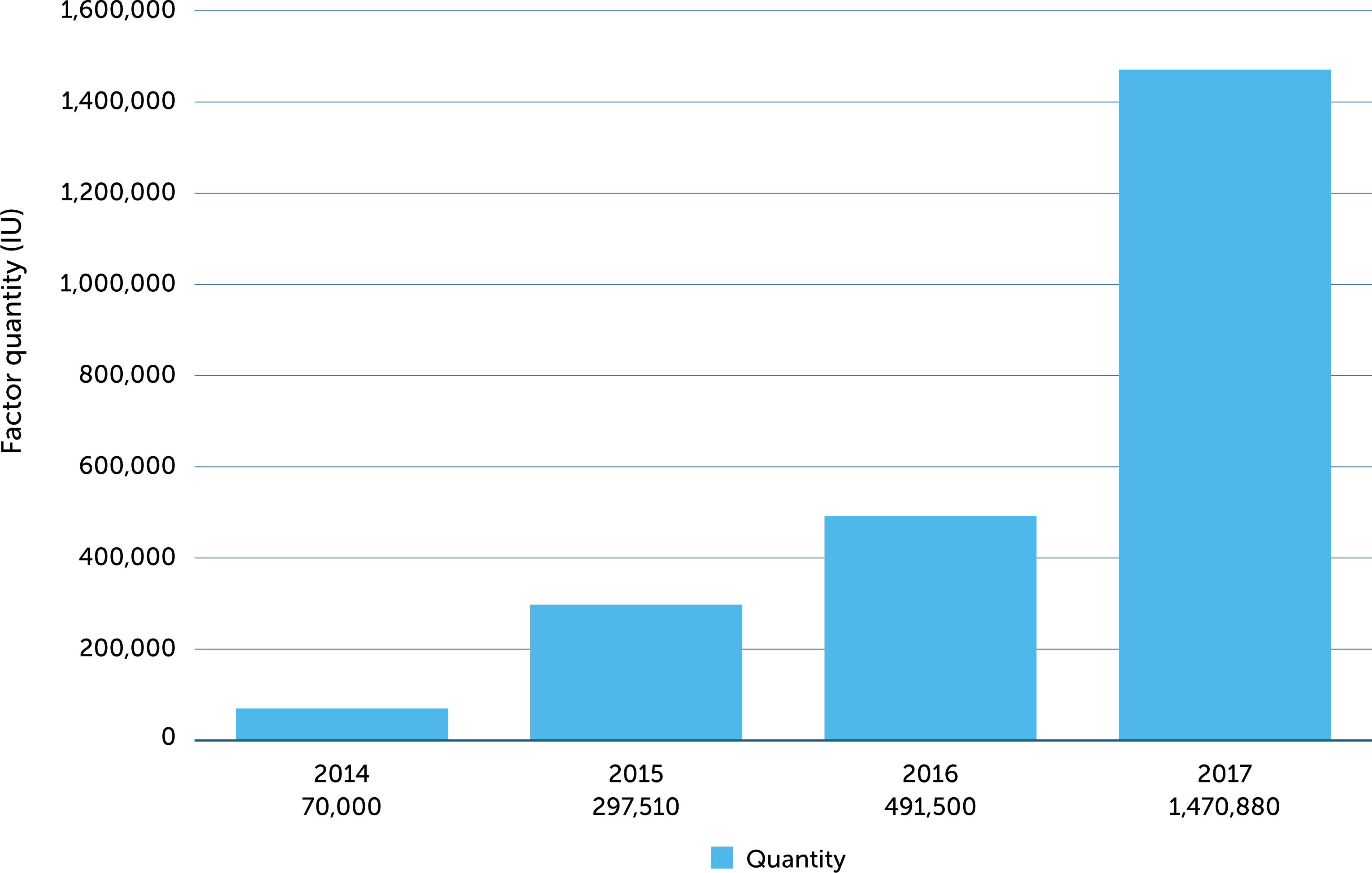
The number of patients registered with the Malian Haemophilia Society increased following the programme. There were 20 registered patients in 2012, 42 at the beginning of the study period in 2016 (26 with haemophilia) and 126 in December 2017. (Some registered patients were referred for tests during the study and are included in Table 1.) This increase was associated with a marked increase in demand for clotting factor concentrates supplied as part of the WFH humanitarian aid programme (Figure 3). This has enabled the provision of low-dose prophylaxis to all patients under five years old, with the potential to improve their quality of life and reduce the risk of joint bleeds and long-term complications.
Impact on the haemophilia social environment
An important direct impact of the programme was the development of collaboration between patients and their families and traditional healers. Involving traditional healers in the detection of new patients is an original approach and an important step in engaging the community to increase awareness.
Progress has also been made in raising awareness of haemophilia among the Malian population more widely. Awareness-raising activities were further strengthened through a WFH twinning programme between the Algerian Haemophilia Association (Association Nationale des Hémophiles Algériens) and the Malian Haemophilia Society in 2017. This resulted in greater media coverage: radio and television stations are now much more interested in awareness-raising activities about haemophilia and other bleeding disorders.
DISCUSSION
The underdiagnosis of haemophilia and other bleeding disorders in developing countries has prompted the WFH to focus its strategy on improving haemophilia care in these areas, through reducing the number of undiagnosed patients, increasing access to treatment, reducing joint disabilities, and generally improving quality of life for PWH [2]. To work on the ground, it is important that any strategy takes into account the realities of the population and their environment. Our approach in Mali was to provide an integrated programme to improve awareness and diagnosis of haemophilia, involving all relevant stakeholders, thereby improving access to care through an innovative strategy based on three pillars:
The identification of social aspects particular to the local population, such as faith, culture and economic capacity
The evaluation of methods, strategies and results reported in the literature about programmes in other countries to ascertain how applicable they are locally, and to avoid any potential conflict of interest
Maintaining relationships with all parties involved to ensure the best outcomes for actions or activities initiated by the programme, based on the best combination of existing and new approaches.
Ideally, this approach is a collaborative model that involves the WFH, laboratories, patients and their families, the government, healthcare providers, and other relevant local stakeholders.
In many African countries, the population continues to approach traditional healers for solutions to problems with their health [16]. Around 80% of the Malian population believe in traditional medicine and use it as the first point of access for the treatment of health issues [16]. In Africa, bleeding diseases are frequently associated with traditional belief and myth, such as offending traditional spiritual laws and witchcraft. Additionally, traditional opinion leaders, including religious and local leaders, play a crucial rule in African society, and their influence can have a positive or negative impact on the popular acceptance of any new idea or project [17,18]. To ensure the successful implementation of a programme that aims to improve haemophilia care in this environment, it therefore is important to take these elements into consideration.
Good collaboration between traditional healers, patient families, opinion leaders and health care professionals during the study led to in an increase in newly diagnosed patients. Improving the knowledge of traditional healers resulted in their involvement in transferring patients from their own offices to treatment centres. Participants in the training sessions had the opportunity to ask questions and did so regularly, which we believe is also an indicator of their success.
The synergy between the WFH and NNHF made it possible to provide training, diagnosis and care for a variety of stakeholders. The training sessions and awareness-raising activities were supported by the NNHF, while diagnostic facilities, drugs for synovitis and clotting factors were covered by the WFH twinning and humanitarian aid programmes. In developing countries with limited resources, such as those found across sub-Saharan Africa, this kind of collaboration has huge benefits for capacity building and improvement in haemophilia care.
Haemophilia is a rare disease which receives little attention in comparison to the tropical infectious diseases prevalent on the African continent. Involving local opinion leaders could be the best way to improve this situation in Africa, as the population is generally more willing to listen to them. Their endorsement could be key to the success of raising awareness of haemophilia and other bleeding disorders.
Implementing haemophilia care in an environment where there is little or no access to treatment is a step-by-step process that requires consideration of local culture, faith and other social aspects if it is to be successful. WFH guidance stresses the importance of patient organisations in developing haemophilia care. This requires a great degree of motivation and, in the context of sub-Saharan Africa, may also carry a risk of stigmatising patients. It is perhaps more practical for health care professionals to take the first steps towards developing and improving the care environment. Following this lead, special research and training programmes, participation in patient meetings, and the advocacy of health care professionals would then enable new patient organisations to grow in such a way that they are sustainable.
CONCLUSION
Capacity building and improving care for haemophilia and other rare bleeding disorders in developing countries can be achieved if the local environment and all relevant stakeholders are taken into account. In the case of Mali, this involved the inclusion of patients and their families, health care providers and traditional healers in a training programme, and an awareness-raising campaign linked with the national media. This has proven to be a successful strategy, resulting in an increase in the number of patients diagnosed with haemophilia and linked to care. As such, it may serve as a beneficial model to follow in other developing countries where haemophilia and other bleeding disorders are under-diagnosed.