Haemophilia affects approximately 1 in 10,000 births globally [1]. The World Federation of Haemophilia 2015 Annual Global Survey identified over 187,000 people with haemophilia; of those identified in higher income countries, 38% had mild haemophilia [2]. Mild haemophilia is defined as 5–40 % of clotting factor activity present [3]. In Canada, haemophilia affects 3710 registered individuals, with approximately 500 males between the ages of 18–34 diagnosed with mild haemophilia [4]. Despite the fact that this is considered a “mild” disease, it is critical to note that many of these young men living with mild haemophilia tend to “neglect” and/or misunderstand the severity of their condition, resulting in serious and avoidable medical situations [5,6,7,8]. These serious medical situations often have a negative impact on the quality of life of these individuals and are associated with tremendous costs to them, their families and the healthcare system [9].
Haemophilia healthcare professionals frequently express frustration that young men with mild haemophilia (YMWMH) seek attention only several days after known trauma [6,7,8,10,11]. Delays in seeking treatment can result in prolonged periods of rehabilitation, utilisation of large amounts of clotting factor concentrates, and increased economic burden on the healthcare system [7]. Impact is also felt by YMWMH due to the social and emotional burdens of missing school and/or work associated with significant bleeds [9,12]. Evidence and clinical experiences suggest that the negative consequences of delays could be avoided if bleeds were recognised earlier and treatment initiated sooner [7,13].
It is paramount for clinicians and researchers to better understand how to support YMWMH in managing their mild haemophilia in ways that fit with their lifestyle. Therefore, this study explored the perceptions of YMWMH on the influence of using the app, HIRT? (Hemophilia Injury Recognition Tool) on their self-management skills when they sustain a musculoskeletal injury.
YMWMH are a particularly high-risk group for unrecognised and unacknowledged bleeds with delayed health care contact [6,7,8,11,14]. Mild haemophilia, unlike severe haemophilia, is often diagnosed later in life following bleeding episodes due to trauma or surgery [15,16,17]. A qualitative study in Canada revealed that YMWMH were reluctant to acknowledge their haemophilia, saying that their condition is “not that bad” [and that they do not perceive their haemophilia as that serious, as compared to those with severe haemophilia [18]. YMWMH are known for not attending their multidisciplinary haemophilia clinic appointments [19]. Many lack the skills to differentiate between serious and benign bleed severity, and they may hesitate to contact the haemophilia treatment centre (HTC) [8,14,18,19]. Injury self-management can be a challenge for YMWMH, not only because of individuals’ reluctance to recognise their haemophilia, but also because of the infrequency of significant bleeds [5,8,12,15,19]. Consequently, clinicians working with these men have recognised the need to provide information and teach appropriate injury self-assessment skills to YMWMH [11,12,14].
HIRT? was developed as an application (app) for smartphones based on the preferences of YMWMH [20,21]. More than 24 million Canadians have mobile devices, with 36% of smartphones used daily by the 18–34 age group [22]. Over 80% of digital time for 18–34-year-olds is spent on apps [23]. Mobile applications are a potentially useful source for providing information for self-care [24]. They are easily accessible, can encourage positive health behaviours , provide specific individualised information, and have the interactive quality of connecting individuals to a health care provider [25,26,27,28]. These features on smartphones allow the “anytime, anywhere” assessments which appear to be particularly important for the YMWMH [29]. As an injury self-management tool, HIRT? was specifically tailored for YMWMH and developed through collaborations between YMWMH, healthcare professionals and computer science experts [30]. Available for free download in both Apple and Google formats since December 2014, the Apple version is again under construction to incorporate new updates and will be newly available September 2017.
Objective
To investigate the perceptions of YMWMH on the influence of the HIRT? app on their self-management skills when they sustain a musculoskeletal injury.
Methods
Research ethics approval was received from the University of Saskatchewan (BEH# 11-300, 31-Oct-2011) and organisational approval from the Saskatoon Health Region (30-Oct-2013).
Young men (18–35 years old) diagnosed with mild haemophilia living in Canada were invited to participate. Purposeful and convenience sampling techniques were used [31]. Recruitment techniques included: an invitation located within the mobile app, advertisement to individuals involved in previous research conducted by the team, postings in the national Canadian Hemophilia Society (CHS) newsletter and webpage, distribution of wallet-sized information cards at haemophilia clinics, and requests to all Canadian HTCs to share information with clinic attendees. Interested participants contacted the principal investigator via the app, by phone or email. Informed consent was obtained, either in-person or electronically. The participants received an interview time and date of their choice. The audio-recorded interviews were conducted in-person or by telephone by one researcher (JN); interviews varied in length from 35 to 65 minutes. Each participant also completed a self-report feedback survey, which was embedded in the app. This was submitted immediately upon completion of the interview to the researcher via the mobile app.
Convergent parallel mixed methods design was used [32]. Qualitative and quantitative data were collected concurrently, analysed separately, then combined to confirm and enhance the credibility of the final interpretation.
Description of HIRT?
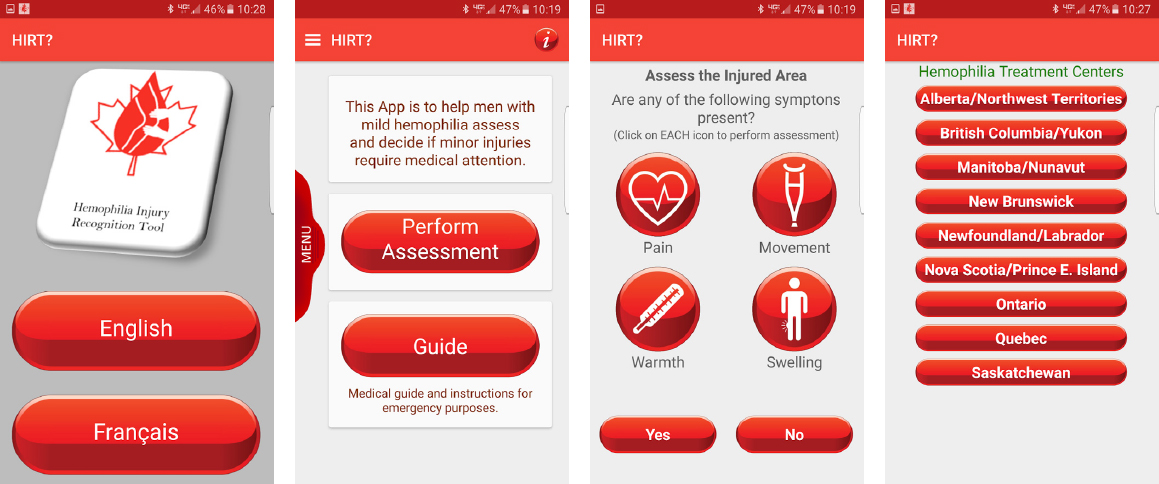
HIRT? is an injury self-management mobile app that asks a series of questions to help an individual assess and identify the symptoms of a bleed which have occurred following a musculoskeletal injury. First aid suggestions are included, with the understanding that in some cases first aid is the only treatment required. HIRT? allows for the delayed onset of symptoms, so users are reminded to recheck the injury at 1 hour, 24 hours and 3 days after first accessing the app. If the symptoms of injury worsen, users are provided with contacts to their local HTC, which can be directly dialled from the app. The app also contains a more detailed assessment guide (see Figure 1).
Quantitative data collection and analysis
Demographic, basic medical and activity status information were collected for each participant at the beginning of each interview, and summarised using descriptive statistics.
Participant confidence ratings for perceived injury self-management were collected during the interviews. These were developed by Graham, allowing individuals with a chronic condition to grade their confidence to complete a desired action in managing their health [33]. Zero was described as no confidence, and 10 the greatest confidence in use of the app to assist skills in injury self-management. The Wilcoxon signed-rank test was used to assess the median differences between the perceived confidence levels of the participant with and without use of the app.
A self-reported feedback survey developed by the researchers was also submitted directly from the mobile app to the researcher’s secure password-locked computer via the web-based data program Apache CouchDB Futon Browse database [34]. The feedback survey included seven variables for bleed assessment and first aid use based on the components present in the app: 1) assessing the injury, 2) ignoring the injury, 3) use of elevation, 4) compression, 5) ice, 6) rest, and 7) contacting the HTC. SPSS was used to analyse the survey results, using a threshold of p <0.05 for significance [35]. The McNemar test was used to assess reported perceived difference with and without use of the app for the dichotomous bleed assessment and first aid use variables, which were analysed individually [36]. The feedback survey also incorporated Likert scales from 0–5 to measure the overall utility of the app, including accessibility, ability to manage an injury, and likelihood of using the app again. Descriptive data were generated, reporting medians, ranges, means and standard deviations.
Qualitative data collection and analysis
An interpretive description approach was used, with the aim of describing a shared circumstance while valuing the experiential knowledge of the YMWMH [37]. This methodology acknowledges that the researcher and the research are inseparable, and is best suited to addressing a clinical concern and allowing the development of knowledge to enhance clinical practice.
The semi-structured interviews, focusing on perceived injury self-management with and without use of the app, were completed from April to July 2015. An interview guide was used to ensure that similar areas were explored with each participant. Two scenarios of musculoskeletal injuries were included in all interviews, assisting those participants who did not use the app for an actual injury. These scenarios were developed by the research team, piloted by YMWMH and deemed to accurately represent a typical injury situation [21].
Table 1
Demographics of participants (n=12)
All interviews were conducted, recorded and transcribed by the same investigator to ensure accuracy and enhance familiarity with the information, then organized for analysis in NVivo, version 10 [37,38]. Inductive content and thematic analysis were used [37,39]. Themes were developed by identifying, reviewing and reporting patterns, then coding and grouping nodes into categories, revising themes and developing a summary.
Trustworthiness of the qualitative analysis was addressed when each participant received, reviewed and confirmed the accuracy of his own interview. Participants were also given the opportunity to review the thematic summary. Dependability of the created themes were confirmed when experts from the research team coded the interviews and compared findings with those of the principal investigator [31]. This occurred in three ways: initially two transcribed interviews were reviewed by two experts, validating the coding techniques used by the principal investigator; next, five experts gave their opinions on the emerging themes; finally, all 12 interviews were reviewed by two expert members of the research team prior to development of the thematic summary.
Results
Twelve participants from six provinces agreed to participate; one individual agreed, but later declined. Due to the infrequency of bleeds in mild haemophilia, only three participants had used the app in a real injury situation prior to their interview [5,8,12,15,19].
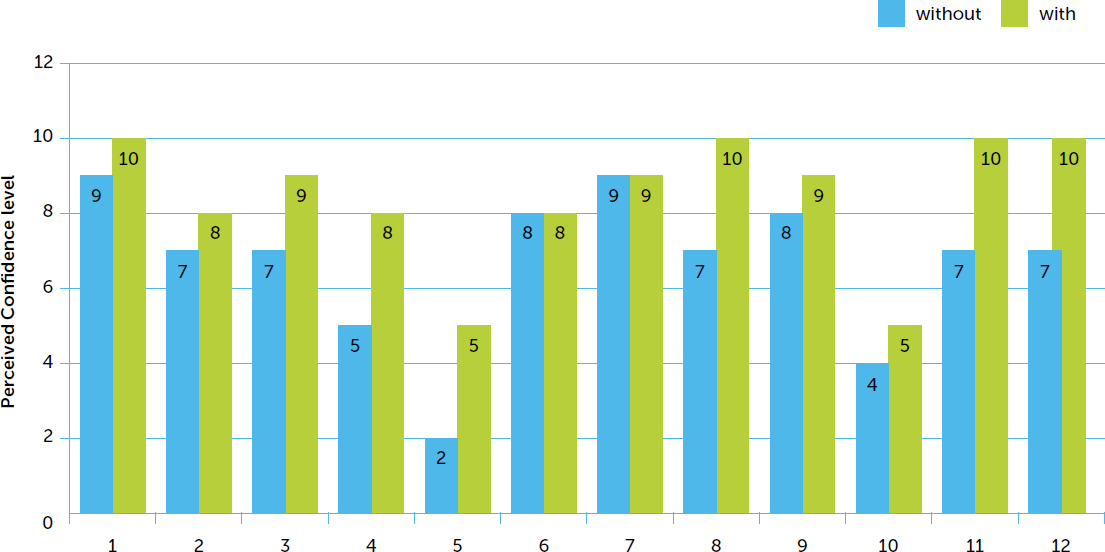
Using the Wilcoxon signed-rank test, a significant overall improvement (p=0.004) was observed in participants’ self-rated perceived confidence to manage a musculoskeletal injury with the use of HIRT? (n=12; see Figure 2).
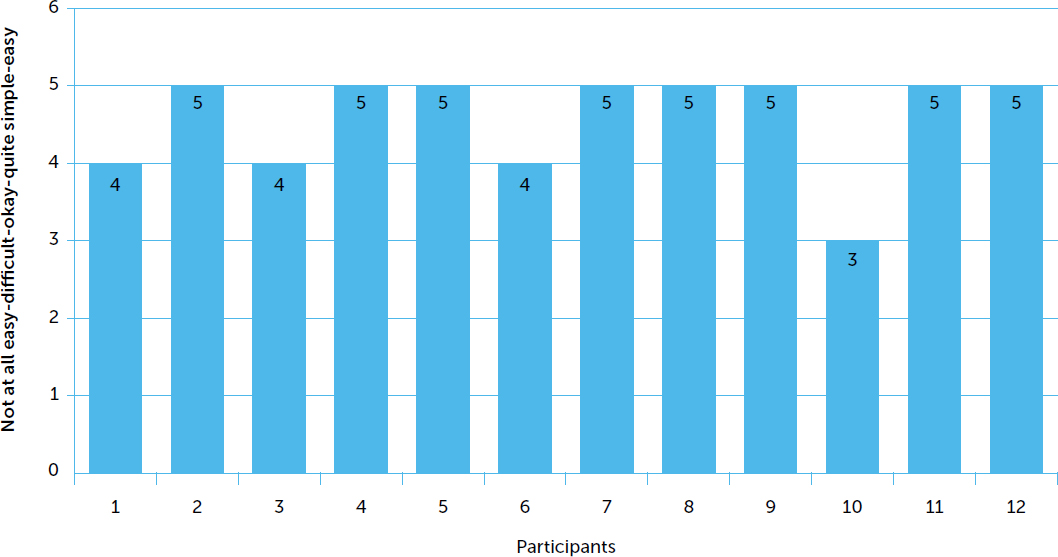
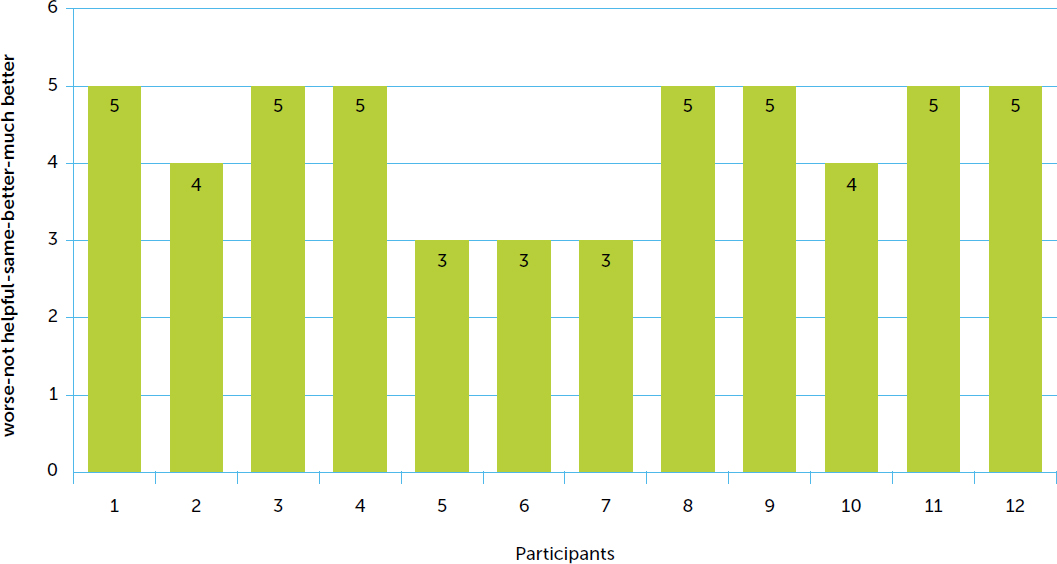
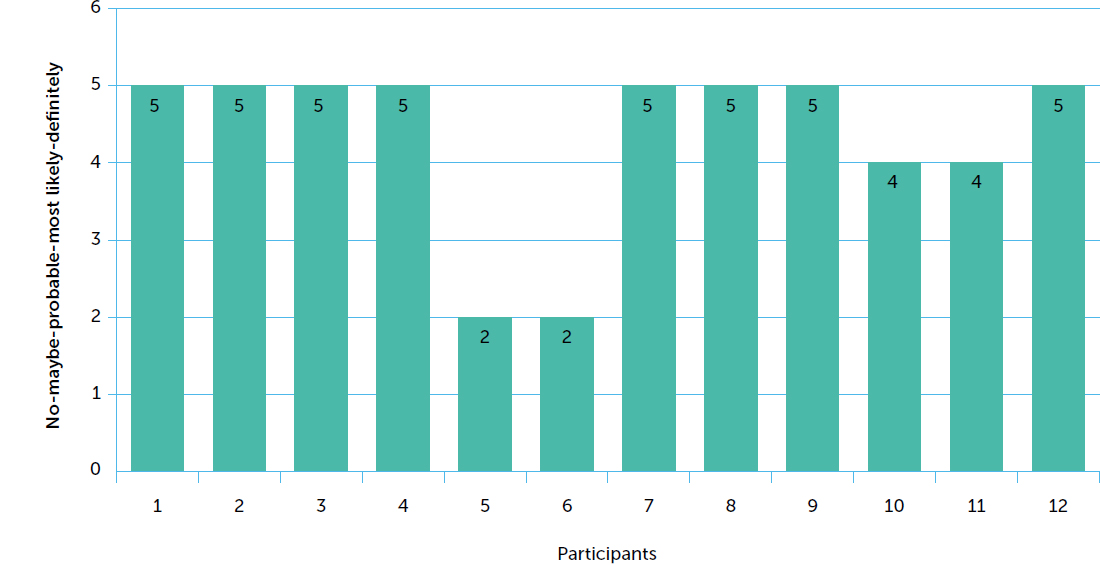
The overall utility of the app was rated mostly positive in the three parameters: accessibility, ability to manage an injury and using the app again (see Figures 3, 4 and 5).
The results of the McNemar test, comparing each of the seven injury self-management variables (bleed assessment and first aid use), on perceived use of the app to no use of the app, found no significant differences.
Five themes emerged from the qualitative data analysis: Accessible, Useful, Alarms, Credible and Confidence.
The participants in this study expressed their excitement in receiving information specifically addressing their needs. Accessibility was acknowledged as “easy”, as evidenced in quotes such as: “I always have my phone handy” and “at your fingertips”.
Three sub-themes were present within the theme Usefulness: Useful to me, Not useful to me and Useful for others. Participants found HIRT? useful for its ability to directly dial the HTC from their smartphones and for the assessment guide. Participants experienced with injuries found the contacts in the app beneficial: “The thing I like the best is all the phone numbers – I just have to tap on it and it just calls it.” With respect to usefulness of assessment guide, one participant stated: “This is the specific information for higher level stuff that I do find helpful.” Those participants less experienced with injuries found the injury assessment parameters gave them a checklist, reminders of things to look for, and reassurance that they had not missed anything. It provided evaluation of an injury that could be done anytime and anywhere, as stated by one participant; “You could sort of do an assessment from the crime scene, really, wherever you get injured.” The young men versed in injury assessment felt that HIRT? would not be useful for them, but felt it would be most useful for others with less experience with injuries, such as younger boys, those living in remote areas, and even parents of children with mild haemophilia.
The alarms, which are a unique feature of HIRT?, prompted the re-checking of an injury. This persuasive technique led the young men through the process of reassessing an injury, then prompted them to call the HTC if needed. One participant stated: “Yes, I think it is important to gauge over time how your body is reacting to the injury, to see how the bleed is progressing or if it is healing at all.” Not all participants had the opportunity to use the reminder system with an actual injury due to infrequent bleeds. The injury scenarios in the interview guide allowed some participants to recognise how the notifications could assist YMWMH to avoid unaddressed injuries. One participant stated: “Milds can deny their haemophilia, and if the app could help me not deny it, it would be really effective.”
The information presented was similar to what the participants had been taught, and was therefore acknowledged by some as credible. One participant commented on similarities with a conversation with his nurse: “I have noticed that her questions are often similar, just like yours are: does it hurt, is there pain, is it warm, have you lost motion.”
Some expressed that the app was “like having someone reaffirm” or “an extra set of eyes”, indicating that it verified their doubts about an injury that was not getting better. HIRT? enhanced their confidence in discussing their injuries knowledgeably with their healthcare professionals.
Barriers related to the use of the app included battery life, misplacing the phone, or being in a location with no phone coverage. Some technical glitches were identified in the reminders to reassess. Some participants also expressed frustration that the app required them to perform the assessment before being allowed to access the rest of the information available through the app.
Recommended improvements were to create a pathway that allowed direct access to the contact numbers and assessment guide, as well as more accurate reminders. Participants who were more experienced with injuries recommended the development of a grading system for symptoms that could provide a more individualised assessment.
Discussion
Many YMWMH find injury self-management a challenge. The HIRT? mobile app offers unique features that support accessibility of information on bleed recognition and management, easy reminders and connections with the relevant healthcare providers [30]. The use of this type of technology for this population of YMWMH has not been previously explored. The YMWMH interviewed in this study unanimously agreed that the format of HIRT? was preferential to paper based educational information on injury self-management.
The mild haemophilia participants in the study by Gamba et al. study were diagnosed at a mean age of 7 years and an age range of 0–35 years, which is similar to other studies [17, 10,18]. The participants in this study were diagnosed with mild haemophilia, with an age range from 0–19 years and median of 6.5 years. The participants also bled infrequently. Many of the participants were less experienced with injuries and appreciated having technology “at [our] fingertips”. Participants perceived that HIRT? could help them make an assessment regarding the seriousness of aninjury. Almost half felt the assessment section of the app would not be useful for themselves, but would be most useful to those less experienced in bleeds or new to haemophilia. However, many of these young men had higher levels of education, and also had more experience with bleeds. This was also reflected through the self-reported data, which did not show any significant difference in bleed assessment or first aid use with or without the use of the app.
HIRT? has the potential to assist YMWMH to take action when they sustain a musculoskeletal injury, as the respondents reported significantly higher levels of confidence in perceived injury self-management when using the app. The app attribute of easy HTC contact has the potential to help YMWMH overcome their resistance to calling healthcare professionals for advice.
The strengths of this study include a mixed method study design which enhances the diversity of results from both quantitative and qualitative data. Another strength was the development of the app and survey tool by experts in the field of haemophilia care in collaboration with the app “users”, i.e. the young men with haemophilia themselves. Integrating the patient voice into the research process enhances the relevance of the research findings. The interviews also provided a venue to solicit ideas for app improvements.
The limitations of this study include a small sample size, use of a survey tool that has not been validated, and the inability to evaluate the use of the app during actual bleeds for all participants. These are areas that can be further explored in future studies.
Significance and Clinical Implications
The mobile app HIRT? is, to our knowledge, the first digital tool informed and evaluated by YMWMH. HIRT? provides a resource to fill a knowledge gap related to improving injury self-management skills of YMWMH, and may also contribute to enhancing overall quality of life and preventing serious medical situations from arising for YMWMH. This tool has the potential to increase self-management skills among YMWMH, reduce the hesitation of the YMWMH to contact the HTC, and decrease the risk of developing serious secondary medical complications post-injury. Those newly diagnosed acknowledged the potential benefit of the assessment and first aid portions. The alarms assisted with prompting reassessment for those who may forget about an injury. Those experienced with bleeds appreciated the assessment guide and HTC contacts. There has been some interest in exploring use of the app in other populations with bleeding disorders, specifically females who are haemophilia carriers presenting with mild haemophilia, and also those on prophylaxis who bleed infrequently. Further research is required to understand the impact of HIRT? in a broader group of people with haemophilia.
Conclusion
Within this study, the HIRT? mobile app had a clinically important and promising influence on perceived injury self-management for YMWMH in Canada. The evidence showed that HIRT? is accessible, easy to use and increased participants’ perceived confidence to identify and manage bleeds. In turn, the use of this tool more broadly by the larger population of YMWMH may, over time, assist in lessening the number of unrecognised bleeds and facilitate earlier communication with the healthcare team. HIRT? was released in December 2014; this is the first study to provide preliminary evaluative data on the tool. Further research to confirm the benefit of this tool for YMWMH will enhance our understanding of its impact.